

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inflammatory root resorption is an unavoidable pathologic consequence of orthodontic tooth movement.1-3 The incidence of root resorption is reportedly 1 - 86% in nonorthodontically treated patients and 19 - 93% in orthodontically treated patients.4 Evaluation of the severity of root resorption requires the establishment of reference data on the normal root length. Early studies5-11 used extracted teeth to derive these measurements, but the difficulty in collecting undamaged extracted teeth always limited the sample size. In many other studies,12-19 periapical or panoramic radiographs were used to measure root length. However, two-dimensional images do not allow accurate measurement: periapical radiographs are distorted depending on the angle between the film and the tooth12-14 and panoramic radiographs show vertical magnification.15-19 Panoramic radiographs are also sensitive to patient positioning; even under optimal conditions, they are fraught with uncertainty, particularly in the anterior jaw regions.20
Cone-beam computed tomography (CBCT) is an alternative technology for evaluating root length or resorption before, during, and after orthodontic treatment. Sherrard et al.21 compared CBCT images and periapical radiographs of extracted porcine teeth to determine the accuracy and reliability of CBCT-based measurements and reported that the CBCT-based measurements of the total tooth and root lengths did not differ significantly from the actual lengths. Further, Lund et al.20 measured root length and the marginal bone level in 13 living patients and 1 dry skull and concluded that CBCT yielded a high level of measurement reproducibility. CBCT-based measurements of patients can be more difficult due to patient movement during imaging.
The purposes of this study were to determine the accuracy of crown and root length measurements of premolars by CBCT by comparing them with direct measurements of subsequently extracted premolars and to provide reference CBCT-based measurement data for the incisors, canines, and premolars of patients with malocclusions. The null hypothesis was that there is no difference in crown, root, and tooth length measurements between CBCT-based and direct measurements.
MATERIALS AND METHODS
This work was approved by the ethics committee of Chosun University Dental Hospital, Korea (CDMDIRB 1218-85). All the subjects gave written consent after the purposes of the study were explained to them.
Assessment of the accuracy of CBCT-based length measurements of premolars
Fifty-two Korean patients who needed premolar extraction were selected from a population of patients who visited the Department of Orthodontics, Chosun University Dental Hospital (Gwangju, Korea) for orthodontic assessment. The premolars were extracted after the patients had undergone CBCT imaging. Among the 152 premolars extracted, 58 were excluded because of the presence of metal restorations, incomplete growth of the root apex or presence of obvious root resorption, presence of a periapical lesion, presence of severe occlusal attrition, or poor CBCT-image quality. Finally, 94 premolars extracted from 21 male (mean age, 22.3 ± 3.0 years; age range, 16 - 30 years) and 21 female (mean age, 20.3 ± 4.1 years; age range, 16 - 33 years) patients were used as specimens.
The teeth were measured by using a digital caliper with a resolution of 0.01 mm (Mitutoyo Corp., Kanagawa, Japan). The following definitions were used for both the direct and the CBCT-based measurements (Figure 1):
In teeth with two apices, the buccal root apex was used for the measurements. Images were obtained using a CBCT scanner (CB MercuRay™; Hitachi Medical systems, Tokyo, Japan) with the following parameters: 149.5 × 149.5 mm field of view, 15 mA, 120 kV, 9.6-s scan time, 0.292-mm isometric voxel size, and 12-bit grayscale.
Measurements were derived from the CBCT images using OnDemand3D 1.0 software (Cybermed Inc., Seoul, Korea). The windowing width and level were set according to the CB MercuRay™ tooth preset (width, 1,726 Hounsefield unit [HU]; level, 870 HU; range, 7 - 1,733 HU) to maintain a constant viewing condition. To enhance edge detection, a color gradient map (rainbow color palette preset) was applied by using the color palette dialog tool under the "fine tuning" tab of the OnDemand3D program. This tool generates color-mapped images according to HU values. The rainbow color palette preset converts pixels over 1,733 HU into red, pixels under 7 HU into purple, and pixels from 7 to 1,733 HU into rainbow colors between red and purple. The alignment procedure of the multiplanar reconstruction windows is depicted in Figure 2.
CBCT-based measurements of incisors, canines, and premolars
The total, crown, and root lengths of the incisors, canines, and premolars were measured by using pretreatment CBCT images of 31 male and 31 female patients with malocclusions. The sample characteristics are shown in Table 1. A preliminary study showed no significant difference between the right and the left teeth; therefore, maxillary right teeth and mandibular left teeth were measured.
The measurement procedures were the same as those used for the CBCT-based measurements in the first part of the study (Figure 2). For the anterior teeth, the incisal edge or cusp tip was used as the reference point instead of the buccal cusp tip. In addition, the root-to-crown (R/C) ratios of the teeth were calculated by dividing the root length by the crown length.
Statistical analysis
All of the measurements of the extracted premolars were repeated after 2 weeks by one investigator (S.Y.K.), and Dahlberg's formula was used to quantify the method error. The Kolmogorov-Smirnov normality test revealed that normal distributions could be assumed for the direct and CBCT-based length measurements of the extracted premolars and the CBCT-based length measurements of the incisors, canines, and premolars. However, when the CBCT-based length measurements of the incisors, canines, and premolars were divided according to gender, the assumption of normal distribution was rejected. The paired t-test and Bland-Altman plots were used to compare the direct and CBCT-based length measurements of the extracted premolars. Pearson's correlation coefficients were used to analyze the relationship between the crown length and the root length of each tooth type. The Mann-Whitney U-test was used to evaluate gender differences. The Kruskal-Wallis test and multiple comparisons were used to test the difference in root length among the tooth types in each gender.
The results were considered significant at p < 0.05. Bland-Altman plots were generated by using MedCalc 12.4.0 software (MedCalc Software, Mariakerke, Belgium), and the other analyses were performed in SPSS 12.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
The method error values of the direct length measurements of the extracted premolars were smaller than those of the CBCT-based length measurements. The method error values of the direct measurements of crown, root, and tooth lengths were 0.18, 0.33, and 0.10 mm, respectively, and those of the CBCT-based measurements were 0.29, 0.82, and 0.28 mm, respectively.
With respect to total length, the CBCT-based measurements were 0.18 ± 0.44 mm shorter than the direct measurements (p < 0.001). However, no significant differences in crown and root lengths were noted between the CBCT-based and direct measurements (Table 2). Bland-Altman plots showed only small mean differences, implying strong agreement (Figure 3). The 95% limits of agreement were -0.90 to 0.90 mm for crown length, -1.23 to 1.18 mm for root length, and -1.04 to 0.68 mm for total length.
The correlation coefficients between crown and root lengths were 0.335 (p = 0.008) for the mandibular canine, 0.264 (p = 0.038) for the mandibular first premolar, and 0.269 (p = 0.036) for the mandibular second premolar. No other significant correlations were evident.
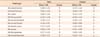
A significant gender difference in the CBCT-based length measurements was noted: the mean crown, root, and total lengths were significantly greater in men (Table 3). However, the R/C ratio showed no significant gender difference (p = 0.807).
The Kruskal-Wallis test revealed significant differences in root length among the tooth types in both the male and female subjects. Multiple comparisons revealed that the maxillary and mandibular canines had the longest roots while the mandibular central incisor had the shortest root in the male subjects; in the female subjects, the maxillary and mandibular canines and mandibular first premolar had the longest roots while the mandibular central incisor had the shortest root (Table 4).
DISCUSSION
When measuring tooth length from periapical radiographs, the likelihood of distortion relative to the projection angle of the X-ray unit should be considered.12,14 Brezniak et al.14 stated that the median CEJ is the best reference point for measuring root length via periapical radiographs. To overcome the drawback of the projection angle in periapical radiographs, R/C ratios were measured in some studies.18,19 In the present study, the buccal CEJ was used as the reference for the crown and root length measurements because it can be located easily on extracted teeth; moreover, in contrast to periapical radiographs, no distortion of the buccal CEJ occurs in CBCT images.
Stratemann et al.22 reported that the differences between direct caliper measurements (the "gold standard") and measurements generated from NewTom and CB MercuRay™ scanning were as low as 0.07 ± 0.41 and 0.00 ± 0.22 mm, respectively. Pinsky et al.23 studied the accuracy of CBCT-based measurements and reported that the mean width and height accuracies for the measurement of intraosseous defects were -0.07 mm and -0.27 mm, respectively. Moreover, Baumgaertel et al.24 investigated the reliability and accuracy of dental measurements on CBCT images of 30 skulls and reported that the compounded measurements of CBCT like required space and available space tended to slightly underestimate the anatomic values. In the present study, the differences in crown and root length measurements were not significant. However, the limits of agreement in the Bland-Altman plot for the root length measurements were wider apart than those for the crown length measurements, ranging from -1.23 to 1.18 mm. This finding means that root length measured by CBCT will differ from the true root length by -1.23 to 1.18 mm in 95% of cases.
Sherrard et al.21 reported that the method error values of tooth measurements increase with the voxel size: in their study, the method error values were 0.266 mm for total length and 0.440 mm for root length when the voxel size was 0.3 mm. Ponder et al.25 also reported that the measurement of root resorption was more accurate when CBCT was performed with a smaller voxel size. In the present study, the method error values of the CBCT-based measurements were larger than those of the direct measurements of the extracted premolars. The CBCT-based measurements of the crown and total lengths exhibited method error values similar to or slightly larger than the voxel size (0.292 mm) used. However, the method error value for root length was nearly three times the voxel size. These findings highlight the difficulty in locating a root apex on CBCT images.
Ozaki et al.10 found that the mean values of all tooth dimensions were greater in male subjects than in female subjects. In the present study, the measurement of every tooth type investigated was significantly longer in the male subjects. Verhoeven et al.6 reported that the central incisor was longer than the lateral incisor in the maxilla and the lateral incisor was longer than the central incisor in the mandible. The total lengths exhibited a similar tendency in the present study, but the mandibular central incisor had the shortest root and maxillary central incisor had the second shortest root, in accordance to the results of Black.5
Weak positive correlations between crown and root lengths were observed only in the mandibular canine and premolars. This result indicates that the root length of patients with malocclusions cannot be estimated accurately from the crown length for most tooth types. The crown measurement was 1.04 mm longer and the root measurement was 0.6 mm shorter in the present study when compared to the Kim et al.26 study on Korean people. This difference might be attributable to the fact that Kim et al.26 measured crown length perpendicular to the long axis of the tooth, whereas it was measured from the cusp tip to the buccal CEJ in the present study. The shorter roots apparent in the present study might be explained by the fact that the sample was comprised of only patients with malocclusions.
Hwang and Song27 evaluated root resorption before orthodontic treatment in patients with malocclusions and reported that the maxillary central incisor was the most susceptible to substantial root resorption. In the present study, the maxillary right central incisor had occlusal contact in 41.9% of the male subjects and 38.7% of the female subjects. The low percentages of occlusal contact might have contributed to the short maxillary central incisor root. To elucidate the relationship between root length and malocclusions, a comparative study of root length in normal occlusion and malocclusions should be conducted. Furthermore, comparisons among various types of malocclusions should be undertaken.
A limitation of this study is that only one HU range was used for reconstructing the CBCT images to maintain a constant viewing condition. This HU range was chosen to highlight the different densities of the root apex and surrounding bone without disappearance of the root apex. If a higher HU range was chosen, the CBCT-based measurements of root length might have been significantly shorter than the direct measurements. Given that the CBCT-based measurements of total tooth length were significantly shorter than the direct measurements, the crown and root lengths may have been underestimated. The measurement of root length is affected by tube voltage and current, voxel size, and grayscale depth during CBCT imaging and the HU range used for image reconstruction. Furthermore, the appropriate HU range for root length measurements can vary greatly when the CBCT scanner or imaging parameters or position is changed because HU values of CBCT are not reliable.28,29 The effect of these factors should be studied in the future. Finally, molars were not measured in the present study because of the need for different alignment during CBCT imaging. Therefore, studies including molar measurements are also required.
CONCLUSION
In this study, CBCT images were obtained using a CB MercuRay™ scanner with a 0.292-mm voxel size and 12-bit grayscale to compare total, crown, and root lengths of premolars measured using CBCT and digital calipers. Because teeth without metal restorations were used as specimens, the results cannot be applied to teeth with such restorations. For total length, the CBCT measurements were significantly shorter than the direct measurements, but no significant differences in crown and root lengths were observed between the methods. Therefore, the null hypothesis was rejected for the total tooth length measurements and accepted for the crown and root length measurements. The method error value of the CBCT-based measurements of crown length was similar to the voxel size used in this study and that of root length was somewhat larger (0.82 mm). In addition, the 95% limits of agreement were wider apart for the root length measurements than the crown length measurements. The data obtained in this study can be used as a reference for evaluating CBCT-based measurements of root length and resorption of teeth without metal restorations in patients with malocclusions.





 XML Download
XML Download