

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The success of orthodontic treatment with fixed appliances depends on several factors, including adequate bracket bonding and the longevity of these accessories on the teeth. In fixed orthodontic therapy, the direct bonding of brackets to the teeth is considered one of the most significant developments in recent decades.1
Other dental treatments, such as with bleaching agents, may affect the bonding ability of the brackets to the teeth. Bleaching agents contain solvents and other components that can increase the solubility or degradation of the bracket adhesive. Additionally, remnants of the bleaching material can possibly interfere with the adhesion and clinical performance of the composite, resulting in decreased shear bond strength (SBS) of the brackets to enamel. It is essential to maintain the biomechanical stability of the bracket-adhesive interface, which transfers the force generated by the archwires to the teeth.2 Bracket loss during orthodontic treatment is the bane of orthodontists and requires additional in-office time and expense to replace the dislodged brackets, as well as extended treatment time in some cases.3,4 Enamel can be lost when the bracket is debonded or during the removal of residual resin. The etching process can also induce irreversible changes to the enamel. In most cases, a rebonded tooth has a weaker SBS than it had when it was initially bonded.5
The effects of bleaching on the enamel surface and the subsequent effect of the composite resin on the SBS have been widely evaluated.6-22 However, the results were quite controversial. Some authors have found no significant differences in SBS between bleached enamel and unbleached enamel.8,9 Then, others reported significant decreases in SBS when bleaching agents were applied.6,7,10-15
The purpose of this study was to test the null hypothesis that no difference exists between at-home bleaching and in-office bleaching on the SBS of brackets bonded with a composite adhesive at 4 different time intervals after dental bleaching.
MATERIALS AND METHODS
Following approval of our investigation by the ethics comittee of Federal University of Pará (protocol, n°185/09), informed consent was obtained from all subjects. For orthodontic reasons, 90 human premolars were extracted from patients aged 16 to 20 years and stored in a solution of 0.9% sodium chloride. Criteria for tooth selection included those with intact buccal enamel, no pretreatment with chemical agents (for example, hydrogen peroxide), no cracks from the extraction forceps, and no caries. The teeth were cleansed of any soft tissue and inserted into polyvinyl chloride tubes (Tigre, Joinville, Brazil) filled with acrylic resin (Vipi Flash, São Paulo, Brazil); therefore, only the crowns of the teeth remained exposed. Each tooth was oriented so its labial surface would be parallel to the force during the shear bond test. The buccal surfaces of the teeth were cleaned with a pumice-water paste in a rubber cup with a slow-speed handpiece for 10 s, washed for 10 s, and then air dried for 10 s.
The specimens were randomly assigned to 9 groups (n = 10) according to the bleaching agents used (at-home bleaching and in-office bleaching) and storage time in artificial saliva (30 min, 1 day, 2 weeks, and 3 weeks) before bonding (Table 1). Specimens in the control group were not bleached and were only immersed in artificial saliva for 1 week before bonding.
At-home bleaching was performed with 7.5% hydrogen peroxide (White Class; FGM, Joinville, Brazil) as recommended by the manufacturer. The bleaching material was applied to the buccal surfaces directly from the syringe and treated for 1 h, after which the specimens were thoroughly rinsed for 15 s and stored in artificial saliva at 37℃. The procedure was repeated for 21 consecutive days.
In-office bleaching was performed with 35% hydrogen peroxide (Whiteness HP Maxx; FGM), according to the manufacturer's instructions. The gel on the tooth surfaces was exposed to a diode emission light (Radii; SDI Limited, Victoria, Australia) for 20 s and left standing for 15 min. After removing the gel with suction, the surface was then washed vigorously and air-dried. The entire procedure was performed 3 times. Following the treatment, each specimen was rinsed in water for 15 s and stored in artificial saliva at 37℃. The bleaching procedure was repeated 3 times with a 7-day bleaching interval.
Ninety standard edgewise stainless steel brackets (Abzil Lancer, São José do Rio Preto, Brazil), each with a 12.06 mm2 surface area, were bonded with the conventional adhesive system, Transbond XT (3M Unitek, Monrovia, USA), according to the manufacturer's guidelines. The bracket was properly positioned on the sample, and each bracket was subjected to a 300-g force. Subsequently, the excess bonding resin was removed using a sharp scaler. Then, a 40-s light-curing method (Radii LED) was performed on the adhesive (10 s on each of the mesial, distal, gingival, and occlusal margins) with an intensity of 1,200 mW/cm2. Thirty minutes after bonding, a universal testing machine (DL 2000; Emic, São José dos Pinhais, Brazil) was used to test the SBS. In order to test the SBS, without touching the enamel and while using a crosshead speed of 0.5 mm/min, a knife-edged shearing blade was positioned parallel to both the labial surface and the bracket interface to allow the transmission of the force in the occlusogingival direction.
The maximum load necessary to debond or initiate bracket fracture was recorded in Newtons and then converted into megapascals as a ratio of Newtons to surface area of the bracket. After bond failure, the same operator (P.S.) examined the bracket bases and the enamel surfaces under a light stereomicroscope at a 10× magnification. The adhesive remnant index (ARI)23 was used to assess the amount of residual adhesive on the enamel surface. The scoring criteria were as follows: 0, no adhesive on the tooth; 1, less than half of the adhesive on the tooth; 2, more than half of the adhesive on the tooth; and 3, all of the adhesive on the tooth.
Statistical analysis
Statistical analyses were calculated using Minitab16 (Minitab, State College, PA, USA). Descriptive statistics including the mean, standard deviation, and the minimum and maximum values were calculated for each test group. The Shapiro-Wilk and Levene tests were used to verify normality and homogeneity, respectively. Analysis of variance (ANOVA) was used to verify intergroup differences because the variables demonstrated normal distribution and homogeneity, followed by Tukey's multiple comparison test. The Kruskal-Wallis test for non-parametric comparison was used to determine significant differences in the ARI scores among the groups. p < 0.05 was considered statistically significant.
RESULTS
The descriptive statistics for the SBS of the various groups tested are presented in Table 2. The results of the ANOVA indicated statistically significant differences among the tested groups (p < 0.0001). The Tukey test showed that the SBS of group 1 (unbleached group) was significantly higher than that of the bleached groups, with the exception of group 2 (bonded 30 min after at-home bleaching), which had a significantly higher SBS than that of group 6 (bonded 30 min after in-office bleaching). We found no statistically significant differences among the other groups. The ARI scores for the all the tested groups are listed in Table 3. The results of the Kruskal-Wallis test showed significant differences among the groups (p < 0.0001).
DISCUSSION
Controversy exists in the literature regarding the effects of bleaching on the SBS of composite resins to the enamel; these results could be attributed to the variability in the bleaching agent concentrations associated with different bleaching protocols, as well as the amount of time allotted between the bleaching and bonding procedures.
Previous studies have examined the physical alterations in the enamel after bleaching as a possible explanation for the change in SBS. The enamel exposed to bleaching agents underwent slight or moderate morphologic surface changes, including increased porosity and decreased microhardness, as well as the loss of mineral content and prismatic form, that resulted in the enamel surfaces appearing to be over-etched.18,19,24 These changes seem to be both time- and concentration-dependent. In addition, it has been proposed that the enamel pores, dentin, and dentinal fluid could theoretically act as a peroxide and oxygen reservoir,11 which results in an oxygen concentration on the enamel surfaces that prevents the complete cure of some resin tags. As compared with the resin tags in the unbleached etched enamel, the resin tags in the bleached enamel that were subsequently acid-etched with 37% phosphoric acid were less defined, more fragmented, and less penetrated, according to prior reports.12,15
In this study, the in-office bleaching groups had lower SBS values than the at-home bleaching groups. This reduction could be explained by the high residual peroxide concentration at the enamel surfaces, as residual oxygen that is released from the bleaching agent may interfere with the infiltration of resin into the etched enamel or inhibit resin polymerization.13,17,24,25 The in-office bleaching method most often uses 35 - 50% hydrogen peroxide, which is considered to have a strength that is 7- to 16-times higher than that of the concentration used in at-home bleaching techniques.16 The increased temperature and higher peroxide concentrations used in the in-office bleaching procedures are designed to accelerate the reaction and produce an immediate effect, probably resulting in significant concentrations of residual peroxide on the tooth surfaces.
Furthermore, in our study, the bleached groups had lower SBS values than the unbleached group, with the exception of the group bonded 30 min after at-home bleaching. This result may be related to the incomplete diffusion of the peroxide into the tooth structure immediately after bleaching. Furthermore, this fact might be associated with the presence of carbopol in the bleaching gel, an additive that thickens the bleaching material, improves adhesion, and prolongs oxygen peroxide release.9 Additionally, such effects could be due to the calcium in the composition of at-home bleaching agents. Calcium ions could increase the bleaching gel saturation and mineral loss, a decrease which occurs during the bleaching action and ion exchange.21 Some authors have found that the addition of calcium to the bleaching agents enhanced the remineralization of the bleached enamel surfaces and subsurfaces.20,22 However, little is known about the effects of remineralizing agents on the enamel; it is possible that 1 day after bleaching, the calcium ions, contained in the gel, are lost from the tooth surfaces.
While taking into account the effect of time between the whitening procedure and bonding, we noted higher SBS values in groups bonded 30 min after whitening compared with 1 day after whitening. In both bleaching systems, we also noted a slight increase in the SBS in those groups bonded 2 weeks after whitening, compared with those bonded 30 min and 1 day after whitening. The SBS returned to values close to those of the unbleached enamel within 3 weeks following bleaching. In the literature, the commonly suggested post-bleaching time ranges from 1 to 3 weeks before bonding.7,8,13,15,16
The increase in SBS over time can be explained by the diffusion and release of oxygen absorbed by the enamel from the external environment.11,24 Once the entrapped peroxide is eliminated, the enamel surfaces may show increased adhesiveness.10 Another possible explanation for the reversal of the low SBS values is the effect of saliva on enamel remineralization after bleaching. Previous investigations have demonstrated that the immersion of in vitro specimens in distilled water, artificial saliva, or even saline solution results in a complete reversal of the reduced enamel bonds.8,10,13 In this study, the samples were kept immersed in artificial saliva during and after the proposed bleaching treatment.
Reynolds1 suggested that minimum bond strengths of 6 - 8 MPa are adequate for most clinical orthodontic needs and are considered able to withstand masticatory and orthodontic forces. In this experiment, the SBS values for all the at-home bleached groups were above this minimum requirement. Thus, bracket bonding after at-home bleaching can be achieved independent of the time allotted after bleaching. However, in-office bleaching necessitates more attention, considering that the SBS values determined 30 min, 1 day, and 2 weeks after whitening were below clinically acceptable tolerances. Therefore, we suggest delaying the bonding procedure for 3 weeks after in-office bleaching.
Borges et al.15 recommended using alcohol-based dental bonding agents to reduce or eliminate the detrimental effects of residual oxygen on the composite bonding process. The high volatility, as well as the solvent and hydrophobic nature of these substances, facilitates the removal of residual oxygen from the tubules owing to rapid evaporation into the environment, thus contributing to increased SBS between the adhesive composite and teeth.15 The primer allows the wettability of the tooth surfaces and permits the substitution of the water retained within the substrate with the resin monomers.26 The bonding agent contains the hydrophobic portion of the system that allows coupling with the resin-based materials. In this context, wettability is a critical factor in establishing an effective adhesion and is related to the intimate contact of the resin in the microporosites of the etched enamel.27 However, the present study showed reduced bond strength values in the bleached groups, even when an alcohol-based adhesive (Transbond XT) designed specifically for orthodontic treatment was used. This observation may be related to the oxidation promoted by the bleaching agent, which reduces the surface energy of the enamel and may also affect the wettability of this substrate by hydrophobic bonding agents.15 If wettability were affected, the resin could penetrate shallower enamel depths and compromise the micromechanical retention necessary for clinical success.
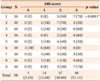
The ARI scores indicated significant differences among the various groups, although ARI scores of 2 and 3 were seen with high frequency. This means that failures occurred at the bracket-adhesive interfaces, as reported in previous studies.9,14 Bracket failure at the bracket-adhesive interface is advantageous as it leaves the enamel surface relatively intact. However, considerable chair time is necessary to remove the residual adhesive and may lead to potential damage to the enamel surface during the cleaning process. However, when the brackets fail at the enamel-adhesive interface, less residual adhesive remains, but the probability of damage to the enamel surface increases.5
CONCLUSION
Despite the limitations of this in vitro study, the following conclusions were drawn.
The null hypothesis was not totally rejected. All the tested bleaching groups had reduced SBS of the brackets to the enamel, with the exception of the group bonded 30 min after at-home bleaching. The in-office bleached groups showed the lowest bond strength values.
All at-home bleached groups exhibited acceptable SBS values. However, when the teeth are bleached with in-office methods, we recommend waiting 3 weeks before bonding the brackets to attain acceptable bond strengths.
The majority of fractures were shown to be adhesive, occurring at the bracket-adhesive interface. However, brackets bonded 30 min and 1 day after in-office bleaching demonstrated a high number of adhesive failures at the enamel-adhesive interface.


 XML Download
XML Download