

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Correction of Class II malocclusions includes growth modification, dental camouflage, and orthognathic surgery. However, dental camouflage with upper first premolar extraction carries the risk of over-retraction of the maxillary incisors and may result in an obtuse nasolabial angle and compromised soft tissue profile, especially if the lower incisors are not proclined to meet the upper incisors in a proper overbite/overjet relationship.1 At the same time, correction of Class II malocclusions can lead to excessive proclination of the mandibular incisors. This is because Class II elastics are often overused as a way to decrease overjet, causing both instability and stress to the labial periodontal support of the mandibular incisors.1 According to Proffit and Fields,2 even in the most favorable circumstances no more than half of the changes needed to correct a Class II malocclusion in an adolescent would be gained by differential jaw growth. It may be assumed that both growth modification and dental camouflage treatments necessitates forward movement of the lower dental arch.
The movement and position of the mandibular incisor play an important role in orthodontic diagnosis, treatment, and management of Class II malocclusions. With this knowledge, the protrusive limits of the lower incisors should be established before treatment, especially in patients with severe skeletal discrepancies3 where incisor movement is limited by the status of the periodontal tissues3 or the anatomy of the symphysis.4 The dimensions of the anterior alveolus also appear to set limits to orthodontic treatment. Challenging these boundaries may accelerate iatrogenic sequelae.5 Thus, the treatment plan should take into account not only the position of the mandibular incisors, but also the morphology of the symphysis. Mulie and Hoeve6 supported this idea by reporting that when the roots of the incisors contacts to the cortical plate of the symphysis, orthodontic movements is inhibited to a greater degree and dehisences or fenestrations may occur.
Several studies have reported differences in alveolar bone thickness or morphology according to facial type.7-9 Handelman5 reported that labial and lingual alveolar widths were small in high-angle subjects as well as in Class III average-angle individuals. Tsunori et al.8 reported correlations between facial type, mandibular cortical bone thickness, and buccolingual inclinations of the first and second molars. Gracco et al.7 stated that the vestibular portion of the cancellous bone of the symphysis is greater in short-face subjects when compared to long-face subjects. According to Swasty et al.,10 mandibular height and width differs more than cortical bone thickness among the 3 types of subjects with different vertical facial dimensions.
With the introduction of cone-beam computed tomography (CBCT) into the field of orthodontics, high-definition images of teeth and surrounding bone can now be obtained at a far lower dose of radiation than that of other medical imaging techniques while being closer to the range of a standard dental film series.11 In conventional cephalometric radiographs, all structures overlap each other because of the divergent nature of the X-ray beam.12 High-resolution CBCT images allow clinicians to visualize the shape and size of the alveolar bones without the disadvantages of conventional radiographs.13 These images are free from distortion and superimposition; thus, CBCT imaging enables quantitative and qualitative evaluation of the relationship between teeth and bone.14 Moreover, CBCT and traditional methods were found to be comparable with respect to linear periodontal defect measurements.15
To date, no study has compared the incisor position and alveolar bone thickness in subjects with Class I and Class II malocclusions by using CBCT imaging. Thus, the aim of this retrospective archive study was to use CBCT imaging (i) to evaluate the alveolar bone thickness of the lower anterior segment and (ii) to determine the parameters that affect lower incisor movement in Class I and Class II average- and high-angle growth patterns.
MATERIALS AND METHODS
Patient selection
Before this study, we estimated the sample size needed to reach statistical significance. Power analysis with G*Power 3.0.10 (Franz Faul, Christian-Albrechts-Universität, Kiel, Germany) showed that 70 subjects would be needed for a statistical power of more than 70% (actual power = 0.7359; critical F = 2.5130; non-centrality parameter λ = 11.200) to detect significant differences with 0.40 effect size and α = 0.05 as the significance level.
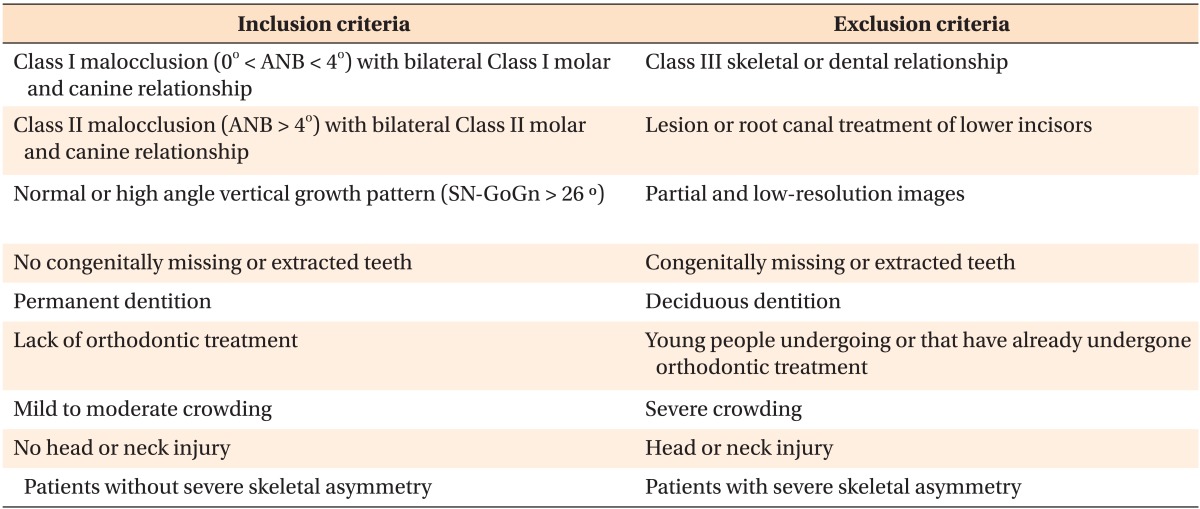
CBCT records were obtained from the archives of Department of Oral and Maxillofacial Radiology, Dicle University (Diyarbakir, Turkey). In this department, records are taken to evaluate implant sites, airway, impacted, missing, or supernumerary teeth, root fractures, bone cysts, dentigerous cysts, abscesses, osteomyelitis, odontomas mucous retention cysts, temporomandibular joints, craniofacial malformations and syndromes. By October 2011, 1,800 sets of images were in the database. Among those 1,800 CBCT scans, 79 were selected according to the criteria described in Table 1. The need for ethical approval was waived because this was a retrospective archive study.
The Class I group was comprised of 41 subjects (18 women and 23 men; mean age, 18.52 ± 5.01 years; range, 11.00 - 32.50 years) and the Class II group was comprised of 38 subjects (22 women and 16 men; mean age, 16.62 ± 4.91 years; range, 10.90 - 30.50 years). The 2 groups were further divided into high- and average-angle subgroups according to the angle formed between Sella-Nasion and Gonion-Gnathion planes (SN-GoGn) angle (the angle formed between the anterior skull base and the mandibular plane).
Cone-beam computed tomography
Tomographs were obtained using CBCT (iCAT, Model 17-19; Imaging Sciences International, Hatfield, PA, USA) with a single 360° rotation and a voxel size of 0.3 mm at the following settings: exposures made with 5.0 mA at 120 kV for 9.6 seconds and an axial slice thickness of 0.3 mm.
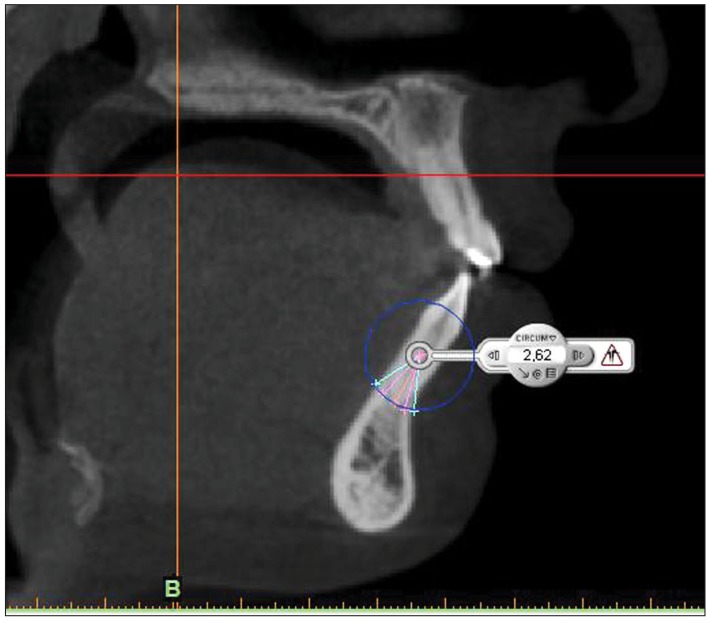
Primary and secondary reconstructions of the data were performed with Mimics software (trial version 14.01) (Materialise, Leuven, Belgium). Secondary reconstruction generates three-dimensional (3D) projections of images with maximum intensity for making linear measurements. For standardization, the right lower central incisor was selected but if any rotation of the right central incisor existed, the un-rotated left lower central incisor was evaluated in sagittal cross-sectional slices at the buccal and lingual surfaces, which were parallel to the midsagittal plane. Before Digital Imaging and Communications in Medicine (DICOM) data was obtained, the midsagittal plane was constructed by NNT viewer software (Newtom QR, Verona, Italy) and the sagittal slice plane of the incisors was established. For sagittal and vertical classification, angle formed between points A, N, and B (ANB) and SN-GoGn were measured by SimPlant Pro 2011 (Materialise NV; Materialise). All the measurements were performed by a single author (F.I.U.).
Landmark identification and measurement
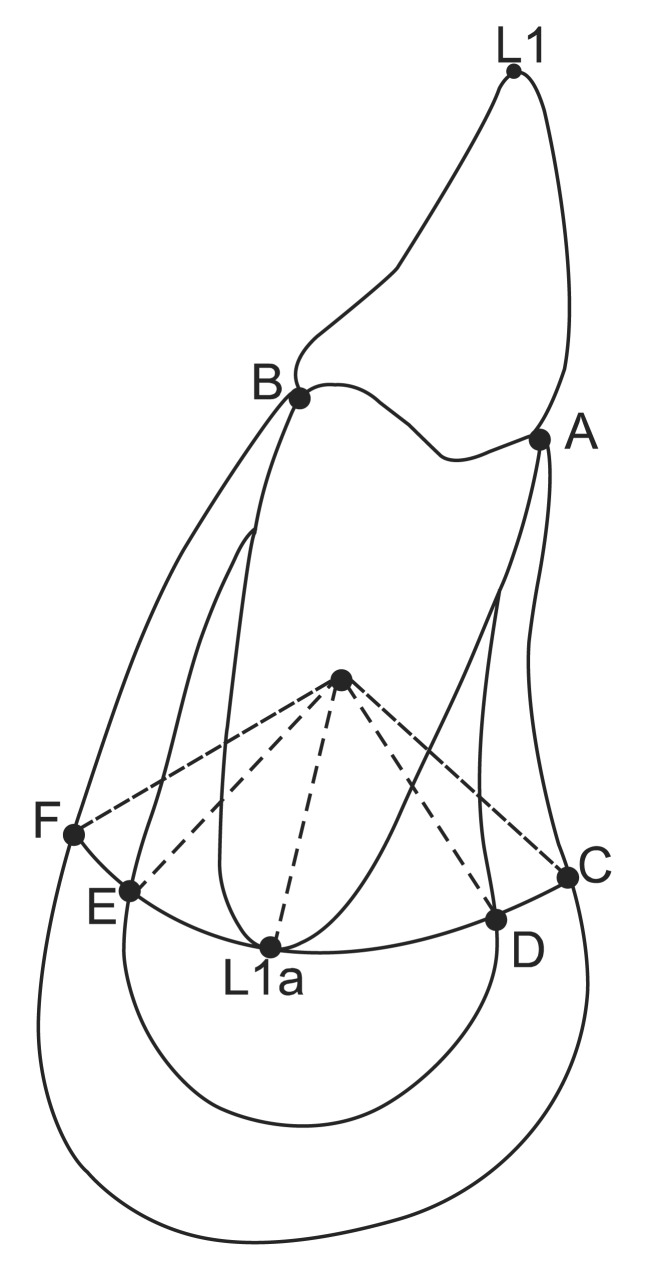
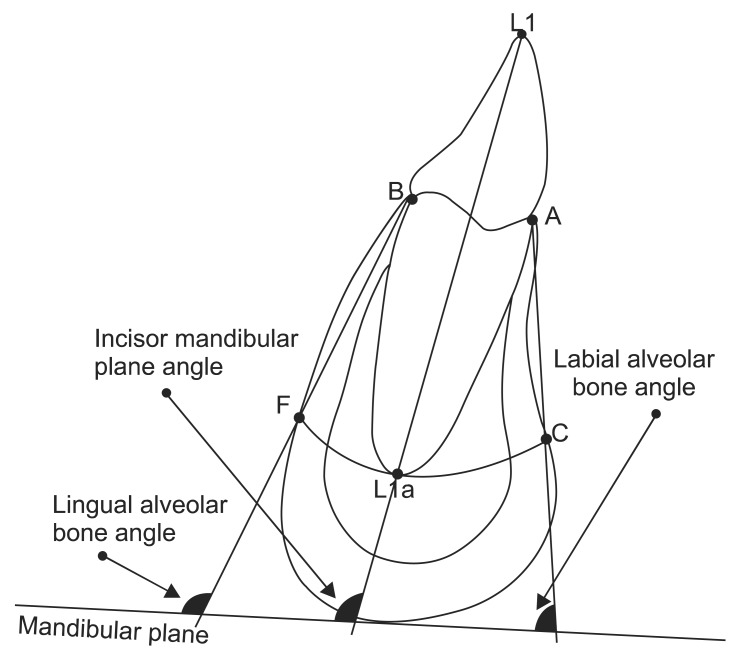
All landmark identifications (Figure 1) and measurements (Figures 2 and 3) were adopted from Yamada et al.12
The center of rotation (CR) was defined as the mid-point of the embedded portion of the root in alveolar bone.16,17 Points A and B were defined as the most anterior-superior point and the most posterior-superior point of the mandibular alveolar bone, respectively. Points C, D, E, and F were defined on the trajectory of the hypothetical tipping movement of the mandibular central incisor root around the CR. Points C and F were defined as the most anterior point and the most posterior point of the mandibular alveolar bone, respectively. Points D and E were defined as the inner contour of the anterior cortical plate and the inner contour of the posterior cortical plate, respectively.
The mandibular plane was defined as the line connecting gnathion and gonion points on the 3D image, which was transferred to the sagittal slices. L1-B perpendicular was the distance between the incisal edge of the central incisor and B perpendicular; this line extends from B point and is perpendicular to the mandibular plane.18 Incisor mandibular plane angle (IMPA) was defined as the angle between the central incisor axis and the mandibular plane. Labial alveolar bone angle was the angle between line A-C and the mandibular plane. Lingual alveolar bone angle was the angle between line B-F and the mandibular line. Labial cortical bone thickness (D-C) was measured as the length of the arc between points D and C. Lingual cortical bone thickness (F-E) was measured as the length of the arc between points F and E. Alveolar spongious bone thickness (E-D) was measured as the length of the arc between points E and D. Alveolar spongious and cortical bone thickness (F-C) was measured as the length of the arc between points F and C. L1a-D was the length of the arc between points L1a and D. L1a-E was the length of the arc between points L1a and E. All linear measurements were measured in millimeters. Linear and angular measurements were performed using Mimics Software (Materialise, Leuven, Belgium) and Screen Protractor software (version 4.0; Iconico, Inc., http://www.iconico.com) on sagitalslices slices.
Statistical analyses
All statistical analyses were performed with SigmaStat 3.1 (SPSS Inc., Chicago, IL, USA). The Shapiro-Wilks normality test and Levene's variance homogeneity test were applied to the data. Parametric tests were applied to normally distributed data (group comparisons) and non-parametric tests were applied to data that were not normally distributed (subgroup comparisons) Arithmetic mean and standard deviation values were calculated for all measurements. An independent samples t-test was used to compare mean values between Class I and Class II groups. The Kruskal-Wallis test and Dunn post-hoc test was used for subgroup comparisons. Statistical significance was tested at α = 0.05.
To determine the errors associated with CBCT measurements, 15 tomographs were selected randomly. Their measurements were repeated 4 weeks after the first measurements. A paired samples t-test was applied to the first and second measurements, and the differences between the measurements were found to be insignificant. Correlation analysis applied to the same measurements showed the highest r-value (0.985) for incisor mandibular angle and the lowest r-value (0.699) for L1a-D measurement.
RESULTS
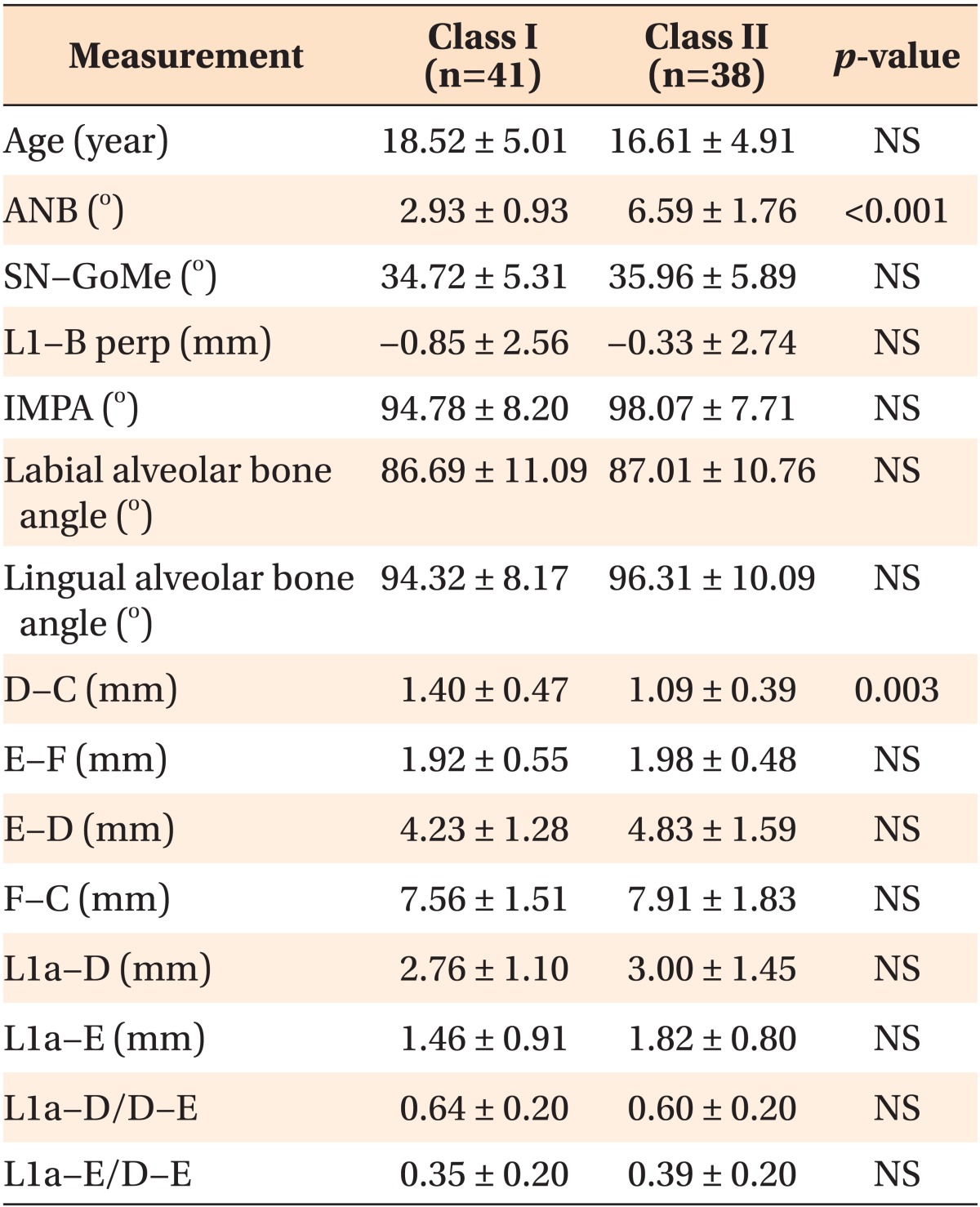
First, we compared lower incisor position and bony support between Class I and Class II groups; descriptive statistics and intergroup comparisons are given in Table 2. No statistically significant difference was found between the 2 groups except for labial alveolar bone thickness, which was higher in Class I than in Class II patients (1.4 ± 0.47 mm versus 1.09 ± 0.39 mm; p < 0.001).
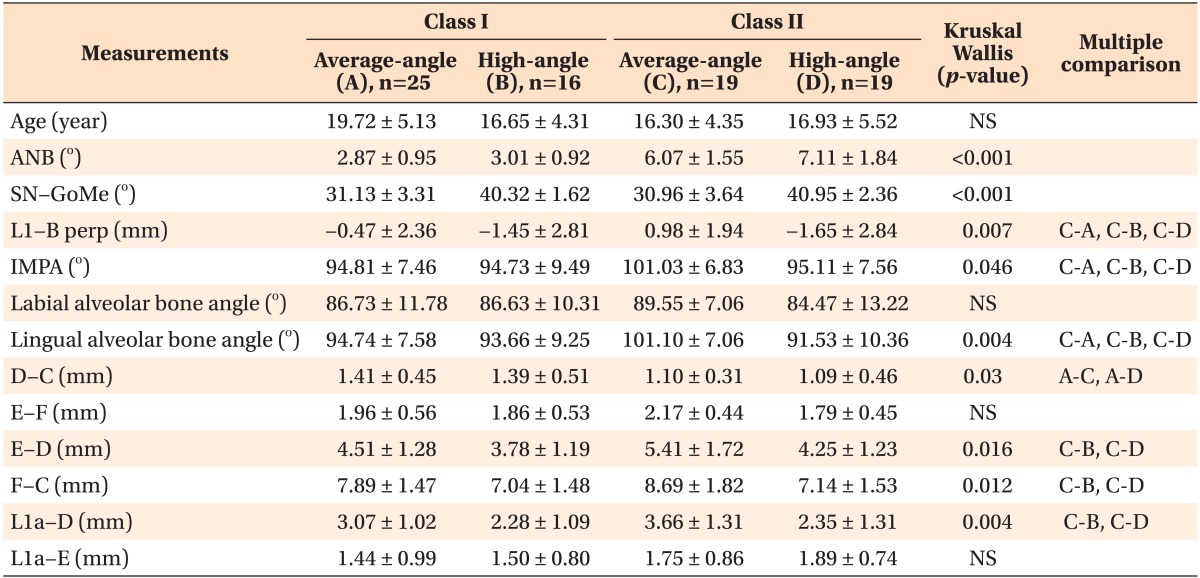
In a second step, we investigated whether differences were more pronounced between average- and high-angle subgroups of Class I and Class II groups (Table 3). Lower incisor protrusion (0.98 ± 1.94 mm; p = 0.007), proclination (101.03° ± 6.83°; p = 0.046) and lingual alveolar bone angle (101.10° ± 7.06°, p=0.004) were higher in the Class II average-angle group than those in other subgroups. Alveolar spongious bone thickness (the arch between E-D), F-C distance, and L1a-D measurements were highest in the Class II average-angle group; the difference was statistically significant between Class II average-angle group and high-angle (Class I and Class II) subgroups (p = 0.016, 0.012, and 0.004, respectively). On the other hand, labial cortical bone was thicker in Class I subgroups compared to Class II subgroups. The difference between Class I average-angle group and Class II subgroups were statistically significant (1.41 ± 0.45 and 1.39 ± 0.51 mm versus 1.10 ± 0.31 and 1.09 ± 0.46 mm in average- and high-angle subgroups, respectively; p = 0.030). The root apex, as measured by the L1a-D distance, was closer to the labial cortex in Class I and Class II high-angle subgroups compared to that of the Class II average-angle subgroup (2.28 ± 1.09 and 2.35 ± 1.31 mm versus 3.66 ± 1.31 mm, respectively; p = 0.004).
DISCUSSION
Teeth may be decentralized from the alveolar bone envelope with orthodontic treatment, depending on the initial morphology of the alveolar bone and the extent of tooth movement.19 The decision as to how much the lower incisors should be moved or how the bone may be affected with tooth movement is a critical consideration in treatment planning. In this study, we showed that mandibular anterior bony support and lower incisor position are different between average- and high-angle Class I and II patients.
Greater differences were found when the groups were subdivided according to vertical growth pattern. It was obvious that in Class II average-angle subjects, the lower incisors were more protrusive and proclined than those of the other subgroups. Nevertheless, increase in lingual alveolar bone angle was found in Class II average angle group. Nevertheless, a positive correlation between the inclination of the incisors and lingual alveolar bone was observed. Similarly, Yamada et al.12 showed a positive correlation between the labial-lingual inclination of the incisors and the alveolar bone on the labial and lingual sides for subjects with Class III malocclusions.
Schudy20 has suggested that the inclination of the mandibular plane is a good indicator of mandibular rotation. In the current study, the mandibular plane angle was used to divide the groups into average- and high-angle subgroups. Bjork21 and Nielsen22 observed that tooth eruption is almost vertical whereas more distal mandibular incisor eruption is characteristic of vertical facial growth patterns. According to the results of the present study, regardless of the basal jaw relationships (Class I or Class II malocclusions), the position and inclination of the lower incisors were similar in the Class I malocclusion subgroups and Class II high-angle group. In other words, the position of the lower incisors differs between average- and high-angle subgroups in Class II, but not in Class I malocclusions.
Labial cortical bone thickness was higher in Class I subjects compared to that of Class II subjects. Thickness of the buccal alveolar cortical bone may increase resistance to bone resorption. This may be especially important when planning treatment for Class II malocclusions, which necessitates incisor protrusion, as the alveolar bone is thin and liable to sustain iatrogenic damage.
E-D and F-C distance measurements are related to cancellous bone thickness of the symphysis. These measurements were greater for the Class II average-angle group. In high-angle subgroups, these values were smaller. As the incisors should be positioned within the cancellous bone, it can be said that the range of movement of the lower incisors in Class II malocclusion subjects is limited in high-angle cases compared to that of average-angle subjects.
The distance between the lower incisor root apex and the inner contour of the labial alveolar cortical bone (L1a-D) showed great variability between groups. In high-angle subgroups, the distance was relatively small. Similarly, Handelman5 and Gracco et al.7 reported that the distance between the apex and the internal surface of the vestibular cortex is greater in short-face than in long-face subjects. On the other hand, L1a-E was not statistically different between groups on the lingual side. However, for all subgroups, the apex-to-vestibular cortex distance was greater than the apex-to-lingual cortex distance. This finding was in accordance with the findings of Gracco et al.7 One could assume that proclination of the lower incisors with tipping may cause damage as the apex of the tooth moves too close to the lingual cortex.
Probing, periapical, or bitewing radiographs and cephalometric radiographs are used for the assessment of bony support.23 However, radiographic methods have some limitations, such as superimposition of the anatomic structures and difficulty in reproducing the angles over time.24 Moreover, underestimation of the amount of real bone loss using radiographic assessment has been reported.13 Cephalometric radiography is a limited tool for the assessment of inclination and thickness of the alveolar bone, especially in the lower anterior alveolar region, because images of all structures overlap in 3D space, thereby giving rise to an important enlargement error due to divergence of the X-ray beam.7 The main advantage of CBCT is its ability to evaluate real anatomy in 3D, true-to-scale images without distortions or superimpositions of the neighboring structures. Furthermore, secondary computerized reconstructions also allow qualitative and quantitative evaluation of bone surfaces, quantitative evaluation of the relationship between teeth and bone,14 and the selection of the desired sections.23
CONCLUSION
Buccal alveolar bone thickness was significantly smaller in Class II than in Class I malocclusion patients.
The lower incisors were more protrusive and proclined in the Class II average-angle subgroup than in other subgroups.
The range of movement of the lower incisors in high-angle Class II patients should be limited compared to that of average-angle Class II patients.
Clinicians should consider vertical facial growth patterns when planning orthodontic treatment.
 XML Download
XML Download