

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Maxillary molar distalization is an increasingly popular option for orthodontic resolution of Class II malocclusions because it enables correction of increased overjet while facilitates space regaining.1,2 Following molar distalization, the premolars, canines, and incisors may be retracted with different techniques.2
Molar distalization appliances can be intraoral or extraoral. Extraoral appliances such as headgear are efficient in improving the jaw relationship,3,4 but they require the patient's cooperation and accuracy during application. In fact, studies on patient cooperation, appliance wearing time, and esthetics5,6 have shown that patient compliance decreases with time7 and that non-compliance is unpredictable.8,9
In contrast, intraoral appliances reduce or even eliminate the need for patient compliance. This has led to the development of many devices such as repulsing magnets,10 NiTi springs,11 the Jones jig,3 pendulum appliances,12 distal jets,13 and superelastic wires,14,15 all of which are efficient in achieving maxillary molar distalization. In 2006, Walde developed an intraoral molar distalizing appliance named the Frog appliance.16 The Frog appliance consists of a special distalizing expansion screw with an anterior activation head that can be easily reached intraorally; additionally, a wired spring is attached to the expansion screw and is inserted into the palatal tubes of the molars. However, intraoral appliances have disadvantages too, including anchorage loss, molar tipping, extrusion with subsequent bite opening, and increased overjet.
To overcome these drawbacks, many researchers have suggested the use of intraoral appliances in combination with uprighting bends, utility arches, and headgear to produce more favorable results, including vertical control of the molars, uprighting of the roots, and prevention of anterior movements of the maxilla.17,18
To date, very few studies have evaluated the efficiency of the recently developed intraoral Frog appliance, and no studies have evaluated the combined use of this appliance with extraoral devices. In this study, we describe the efficiency of the Frog appliance - alone or in combination with headgear wear - in achieving maxillary molar distalization.
MATERIALS AND METHODS
Patient selection
Before undertaking this randomized clinical trial, we estimated the sample size required to achieve statistical significance. Power analysis using the Minitab software (version 15; Minitab Inc., State College, PA, USA) showed that 19 subjects per group would be required to achieve a statistical power of 90% at a significance level of 0.05. We increased the number of subjects per experimental group up to 25 to cover possible withdrawals. The research sample consisted of 50 patients (25 males and 25 females) with a mean age of 14.3 ± 1.8 years (range, 12.6 - 16.7 years) who sought treatment at the Orthodontic Clinic of Al-Baath University (Hama, Syria).
All the patients had Angle's Class II malocclusion resulting from dentoalveolar deformities or simple skeletal discrepancies in the maxilla. All patients had an ANB angle ≤5°, and they were chosen based on the following criteria: permanent occlusion with fully erupted second maxillary molars; sufficient posterior space for the molars, according to Ricketts et al.;19 the presence of third molar buds, which have erupted only to the level of the middle of the roots of the maxillary second molars; a well-aligned mandibular dental arch, with minimal crowding; normal or horizontal growth pattern; acceptable facial profile (not requiring modification); no history of previous orthodontic treatment; absence of extraction in the treatment plan; and adequate oral hygiene.
After ensuring that the inclusion criteria were fulfilled, informed consent was obtained from the patients' parents after acquainting them with the aims of the research and the relevant procedures.
A computer-generated randomization list was used to randomly divide the patients into 2 equal groups of 25 patients each. Group 1 was treated with the Frog appliance (Forestadent, Pforzheim, Germany) alone, while group 2 was treated with the Frog appliance in combination with high-pull headgear worn at night (Table 1, Figure 1). Both the patients and the researcher were aware of the allocation during treatment, but the researcher was kept blinded during data analysis, as described below. Distalizing appliances were not combined with any other appliances during this stage of the treatment.
The Institutional Review Board approval was achieved for this research.
Frog and headgear appliances
The Frog appliance kit consists of a special expansion screw that is activated anteriorly by using a special key. It also contains a prefabricated palatal arch that has been adapted to fit the posterior end of the expansion screw (Figure 2).
To fix the appliance, wiry spurs were used on the maxillary first premolars, and bands were used on the maxillary second premolars. The parts of the appliance were gathered with an acrylic button based on the palate. The opening of the expansion screw pushes the palatal arch distally, leading to distalization of the maxillary molars (Figure 3).
In group 2, besides the Frog appliance, face bows were applied to the buccal tubes of the maxillary first molar bands with high-pull headgear, which was only used at night (Figure 4).
Treatment continued until Class I occlusion with an overcorrection of 2 mm was achieved (Figure 5).
All appliances were then removed, and records were obtained immediately.
Cephalogram image analysis
Pre- and post-treatment lateral cephalograms were obtained in centric occlusion.
Important skeletal and dental changes were studied. SPP (the line drawn between the anterior nasal spine and the posterior nasal spine; constructed X-axis) and PTV (the perpendicular line to Frankfurt plane through Ricketts' pterygoid point; constructed Y-axis) lines were drawn. The constructed X-axis was used to describe vertical and angular measurements, whereas the constructed Y-axis was used to describe sagittal measurements. The incisal edges of the central incisors and the central points of the crowns of the molars and premolars represented the middle points of the lines that connected the mesial and distal maximum convexities of the crowns (Figure 6). Angular changes were measured using teeth axes that were perpendicular to the lines that connected the mesial and distal maximum convexity points of the crowns (Figure 6).
During cephalogram image analysis, the researcher was blinded to the identity of the patients, i.e., pre- and post-treatment cephalograms were analyzed after replacing the patients' names with codes.
To determine the error associated with the method used for cephalogram image analysis, 10 randomly selected cephalograms were traced at least 1 month after the first tracing, and separate sheets were used to collect the new data.
The total method error (ME) was calculated using the Dahlberg equation:20
where d is the difference between the 2 measurements and n is the number of duplicate measurements. The ME never exceeded 0.4 mm or 0.5°.
Statistical analysis
For determining the changes induced by the appliances in each group, we tested the null hypothesis, which suggested that there would be no significant changes associated with the use of the Frog appliance, nor with its combination with high-pull headgear. For determining the differences between the 2 groups, we tested the null hypothesis, which suggested that there would be no significant differences between the 2 treatments.
All variables were obtained on pre-treatment cephalograms (T1) and post-treatment cephalograms (T2). The data were then entered into SPSS 17.0 (SPSS Inc., Chicago, IL, USA) to process pre-treatment variables, the treatment effects on the studied variables in each group, the relationship between the used appliance and the amount of changes in the studied variables, treatment time, distalization speed, and the ratio of maxillary molar distalization movement relative to the overall opening space between the first maxillary molars and second premolars.
Paired-sample t-tests were used to determine the significant changes induced by each treatment, and 2-sample t-tests were used to compare the differences between the 2 treatments. All the results were judged at a 5% confidence level.
RESULTS
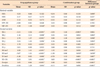
First, we determined whether the 2 groups were similar at baseline. The 2-sample t-test showed that p-values were greater than 0.05 for all the studied variables, that is, at the 95% confidence level, there were no statistically significant differences in any variable before treatment (Table 2). These results indicated that the 2 groups were equivalent.
Then, we used a paired-sample t-test to determine the effects of each type of treatment; we also employed a 2-sample t-test to compare treatment efficacy between the 2 groups (Table 3). The maxillary molars moved distally by 5.51 ± 2.56 mm and 5.93 ± 1.46 mm in groups 1 and 2, respectively. The change was significant in each of the 2 groups (pre-versus post-treatment), but there was no significant difference between the 2 groups.
Molar distalization was associated with tipping of molar axes by 4.96 ± 1.41° and 1.25 ± 2.02° in groups 1 and 2, respectively. The tipping was only significant in group 1, and it was significantly larger in this group than in group 2 (p < 0.001).
Mesial movement of the second premolars was 2.70 ± 1.37 mm and 0.90 ± 1.38 mm in groups 1 and 2, respectively. Although the change was significant in each of the 2 groups, mesial movement was significantly higher in group 1 than in group 2 (p = 0.008).
Two-sample t-tests were used to study the differences in overall treatment time, speed of maxillary molar distalization, and the ratio of the maxillary molar distalization movement relative to the overall opening space between the molars and second premolars between the 2 groups (Table 4).
Treatment time was significantly greater in group 1 than in group 2 (7.44 ± 1.30 months versus 6.27 ± 1.11 months; p < 0.001). The speed of maxillary molar distalization was also significantly lower in group 1 than in group 2 (0.68 ± 0.40 mm/month versus 0.86 ± 0.32 mm/month; p < 0.001). Finally, the ratio of the maxillary molar distalization movement relative to the overall opening space between the molars and second premolars was significantly lower in group 1 than in group 2 (70.74% ± 7.25% versus 90.97% ± 5.51%; p < 0.001).
DISCUSSION
In this study, we showed that the intraoral Frog appliance is an effective tool for promoting maxillary molar distalization, even more so when used in combination with extraoral high-pull headgear. A review of the orthodontic literature reveals the lack of studies that have tested the efficiency of the Frog appliance, with only one case report published.21 Another study presented 2 case reports for the application of a modified Frog appliance, the so-called skeletal Frog appliance.16 No study has hitherto tested the effectiveness of the combined Frog appliance and headgear; this hinders the comparison of the present results with previously reported data.
In this study, the Frog appliance - alone or in combination with headgear - significantly promoted the distalization of the maxillary molars. Our displacement values were similar to those obtained by Chiu et al.22 and Bussick and McNamara23 using the pendulum appliance (6.10 mm and 5.70 mm, respectively). However, our values were greater than those obtained by Bayram et al.21 with the Frog appliance (4.00 mm), Bondemark and Karlsson2 with headgear (1.00 mm), and Patel et al.24 with the Jones jig appliance (3.20 mm). These differences may be due to the longer duration of the present treatment as well as its endpoint (the attainment of overcorrection).
Tipping of the molar axes using the Frog appliance alone was similar to that obtained by Chiu et al.22 with the distal jet (5.00°) and by Kinzinger et al.25 with the pendulum K (4.65°). Bussick and McNamara23 and Patel et al.24 achieved better tipping with the pendulum (10.60°) and the Jones jig (9.54°). These differences may be due to the differences in appliance design and in the point of force application relative to the center of resistance of the molars. However, the molar tipping found in the current study was greater than that in the studies by Bayram et al.21 and Bolla et al.1 (3.00° with the Frog appliance and 3.10° with the distal jet). In addition to the difference in appliance design, these differences may have resulted from differences in the extent of molar distalization.
The amount of molar tipping associated with molar distalization was lesser in the combination group than in all previous studies. This may be due to the uprighting of the molars, accomplished by the high-pull headgear, which may have contributed to adjust distalization-associated tipping.
Premolar mesial movement values found in the present study in the Frog appliance group were similar to those found by Chiu et al.22 with the distal jet (2.60 mm), and by Ghosh and Nanda12 with the pendulum (2.25 mm). However, the values were higher than those found by Chiu et al.22 with the pendulum (1.40 mm). These differences may be due to differences in the extent of molar movement, which is positively proportional to the amount of anchorage loss. The design of the appliances may also play a role.
Premolar mesial movement was lesser in the group that underwent treatment with combined Frog appliance and headgear. This may be due to the influence of the headgear itself, which may adjust the mesial forces applied to the premolar teeth by the Frog appliance. However, in other studies that used only headgear to achieve molar distalization, the premolars moved distally, such as in the study by Brickman et al.26 with cervical pull headgear.
Despite the lack of significant skeletal changes in the sagittal plane in both studied groups, some significant differences were noted between the 2 groups. A slight progress in point A and a non-significant increase in the ANB angle were observed in the Frog appliance group, while a slight decline in point A and in the ANB angle were observed in the combination group, leading to significant differences between the 2 groups.
The associated skeletal changes in the vertical plane were evident in the posterior rotation of the mandible in the Frog appliance group; this resulted in significant differences in mandible position between the Frog appliance group and the Frog appliance plus headgear group.
In the current study, the combination of the Frog appliance and the application of high-pull headgear at night was able to reduce the time required for maxillary molar distalization, with an average treatment time of 7.44 months and 6.27 months in the Frog appliance group and the combination group, respectively. These results are similar to those obtained by Ngantung et al.27 with the distal jet (6.70 months) and to those by Bussick and McNamara23 with the pendulum (7.00 months). However, the average treatment time was greater than that in the studies by Bolla et al.1 with the distal jet (5.00 months) or by Haydar and Uner3 with the Jones jig (2.50 months). These differences may be due to the greater molar movement observed in the current study and the differences in appliance design.
CONCLUSION
The Frog appliance effectively distalized the maxillary molars in patients with Class II malocclusion and fully erupted second molars. This distalization was associated with an acceptable degree of loss of anchorage and with some unfavorable changes, such as axial tipping of maxillary molars, mesial movement of the anchor teeth, and backward rotation of the mandible.
Nighttime application of high-pull headgear together with the Frog appliance can greatly reduce or even eliminate most of these unfavorable changes. The combined use of these 2 appliances can also reduce treatment time, increase the speed of distalization, and improve treatment outcomes by increasing the ratio of maxillary molar distalization movement relative to the overall opening space between the first maxillary molars and second maxillary premolars.









 XML Download
XML Download