

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Moyers1 defined retention as "The holding of teeth following orthodontic treatment in the treated position for the period of time necessary for the maintenance of the result." To date, several retention devices have been used after orthodontic treatment in order to maintain arch form and minimize the possibility of relapse. Despite the increasing popularity of lingual retainers, the advantages of removable appliances for both the patient and the orthodontist have ensured the continuing relevance of these appliances. The Hawley retainer, which was designed in 1919 by Charles Hawley2 and has been used for nearly a century since, is the most popular removable retention appliance. In 1993, Sheridan et al.3 introduced the Essix appliance (DENTSPLY Raintree Essix Glenroe, Sarasota, FL, USA) as an esthetic, comfortable, and inexpensive modern alternative to traditional retainers. Currently, both Essix and Hawley retainers are frequently used in orthodontic practice.
Several studies have investigated the characteristics, advantages, and disadvantages of various types of retainers. However, Hawley-type retainers, which are used by clinicians worldwide, have not been investigated in detail.4-8 Similarly, a limited number of studies have investigated the retention characteristics of Essix retainers. Sheridan et al.3 suggest that the retaining component of Hawley retainers is insufficient for anterior teeth because the retainers have a point contact wire on the labial surface and a mass of acrylic approximating the lingual cervix. However, the Essix appliance completely encapsulates the dentition and the superior part of the alveolus, thus providing better retention. Some studies have compared these appliances in terms of their cost effectiveness, patient satisfaction, occlusal contact pattern, and articulation of speech during retention.7-10 Other studies have evaluated the clinical effectiveness of these retainers.11,12 These studies compared Essix and Hawley retainers for the first 6 months of active retention; however, they did not compare any changes during the follow-up period.
We aimed to compare the clinical effectiveness of Hawley and Essix retainers for a 1-year retention period and to observe the stability of the teeth after a 2-year follow-up period.
MATERIALS AND METHODS
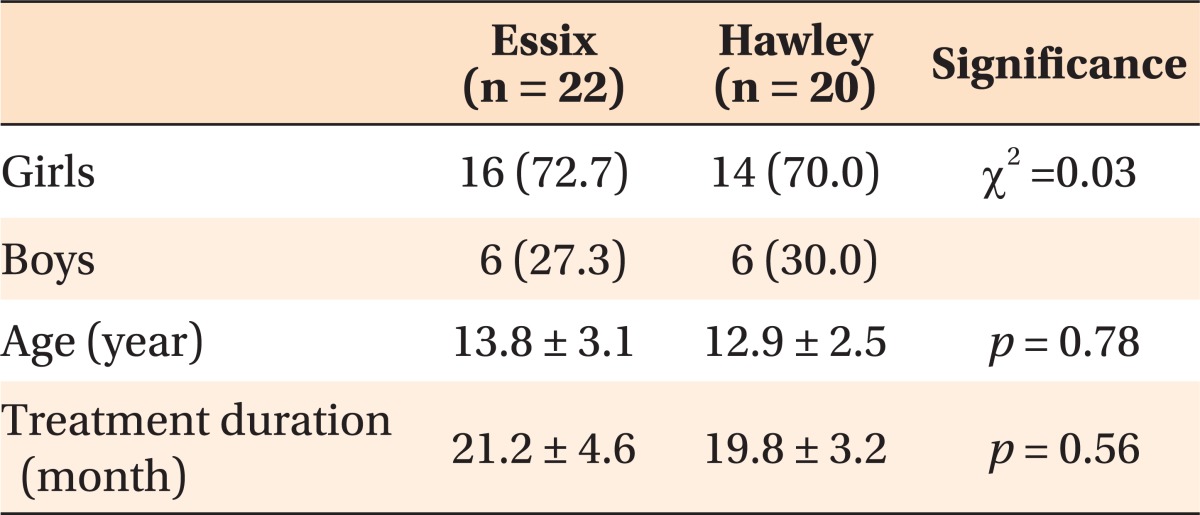
Forty-two patients who had completed fixed orthodontic treatment from the postgraduate orthodontic clinic at the Faculty of Dentistry at Selcuk University and Cumhuriyet University were included in the study. Ethical approval for this study was obtained from the Ethics Committee of the Faculty of Dentistry at Cumhuriyet University. Two experienced orthodontists (AD and HB) treated all the patients between 2002 and 2006. Patient inclusion and exclusion criteria were as follows: no previous orthodontic treatment, normal skeletal and dentoalveolar sagittal, vertical, and transverse relations, and dental Angle Class I or slight Class II molar relation. A non-extraction treatment protocol was approved for all patients with straight wire appliances (0.018-in slot, Roth prescription). During treatment, interproximal stripping to correct crowding and interarch size discrepancies was used when necessary. In this study, 22 patients (16 women and 6 men) received Essix retainers while 20 received Hawley retainers (14 women and 6 men). The mean treatment time was 21.2 ± 4.6 months for the Essix group and 19.8 ± 3.2 months for the Hawley group. A power analysis showed that 20 patients per group would be sufficient (α = 0.05, and power [1-β] = 0.80). The mean retention time was 1 year, and the mean follow-up recall time was 2 years for both groups. Table 1 presents the demographic characteristics of the study participants.
The lateral cephalograms and dental casts obtained at the pretreatment (T1), posttreatment (T2), postretention (T3), and follow-up (T4) stages were used to assess the differences between the Essix and Hawley retainers. These measurements and analysis were performed by the same examiners who were blinded to the experiment (RN and TT).
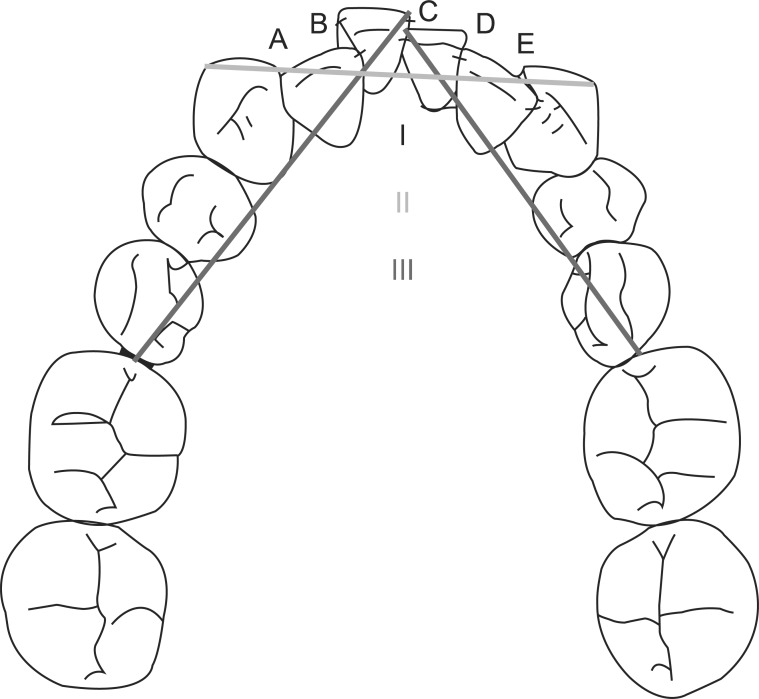
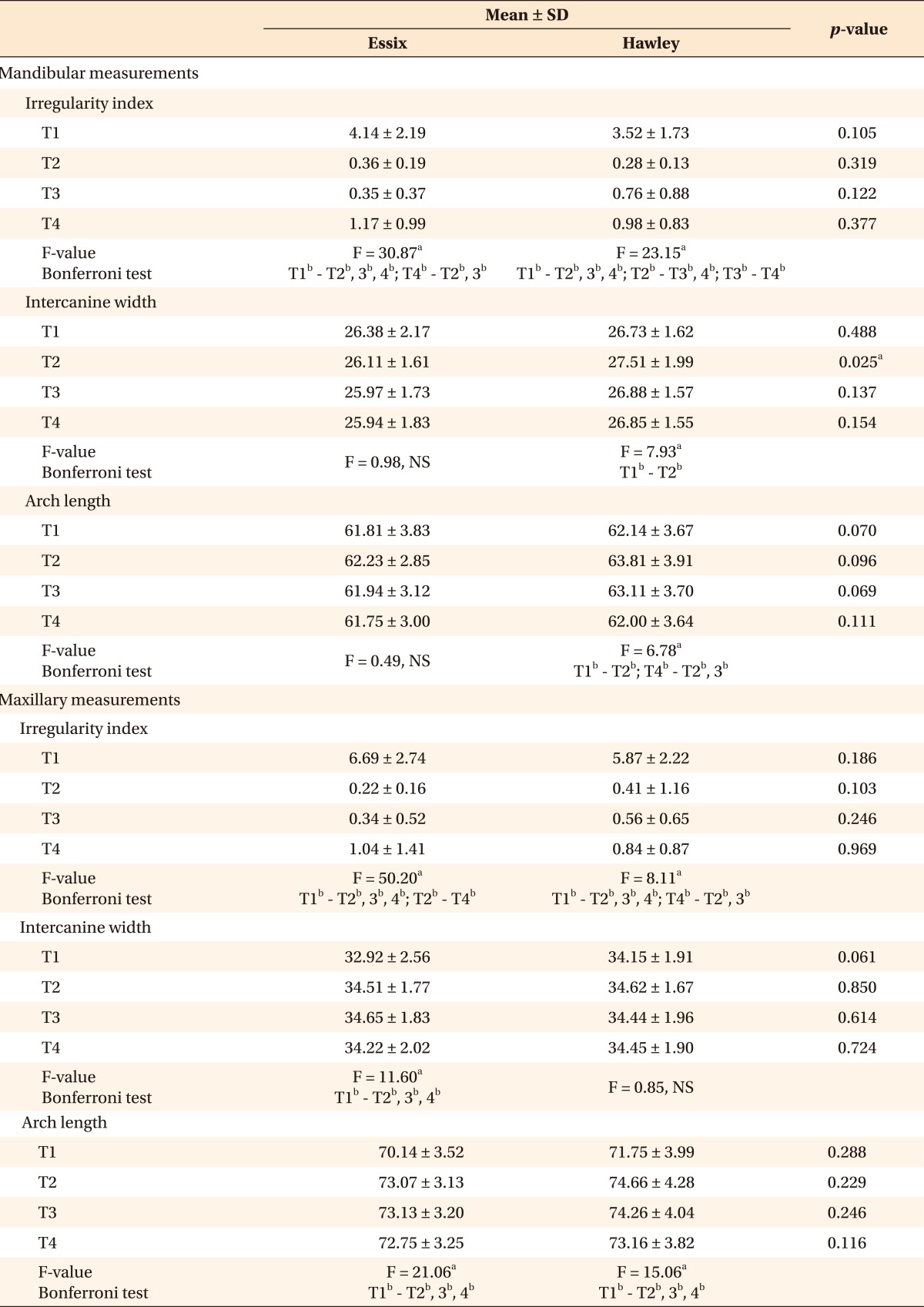
Vernier calipers (precision: 0.1 mm) were used to measure the dental casts. The irregularity index,13 intercanine width, and arch length of the maxillary and mandibular arches were measured on the dental models (Figure 1). The differences in these variables at posttreatment and postretention stages were evaluated to determine the success of the 2 retainers. Any change in these variables from the posttreatment to the follow-up stage was considered a relapse.
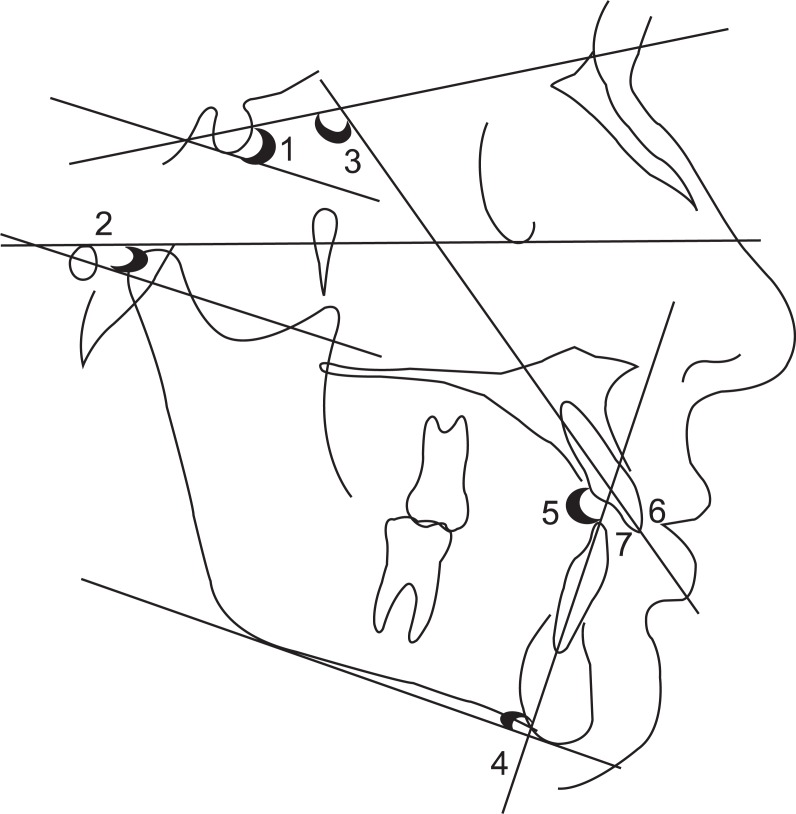
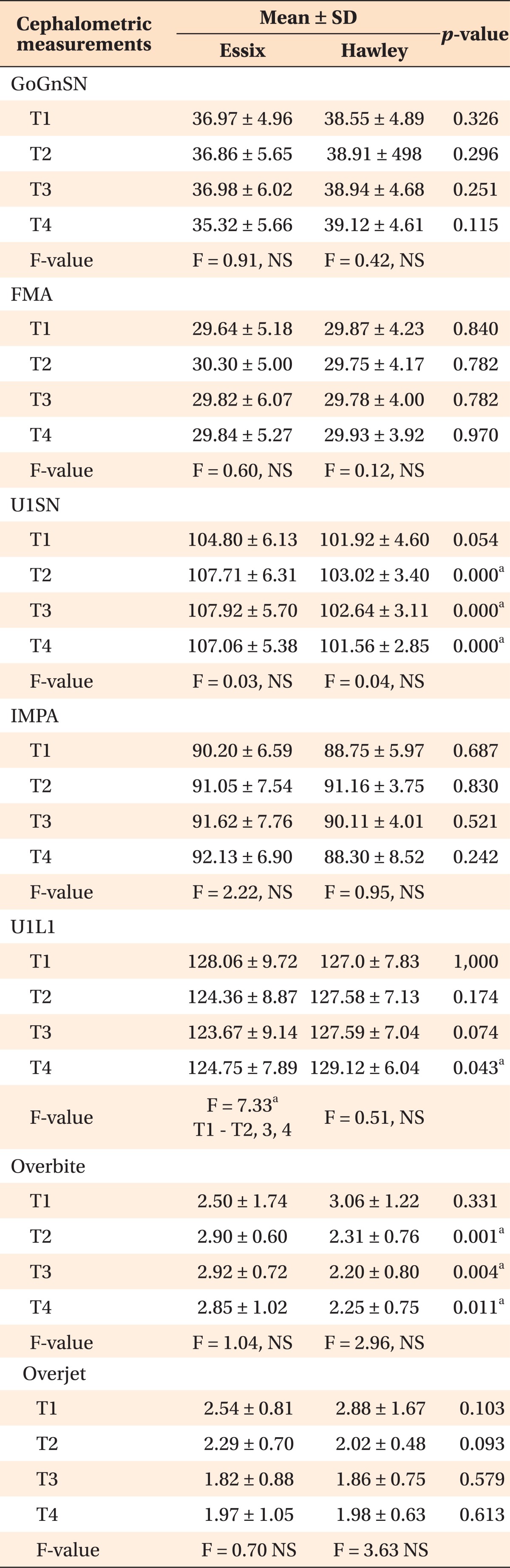
The potential movements of incisors and vertical skeletal changes were evaluated on the lateral cephalograms. Lateral cephalograms were obtained using the same radiographic equipment (Proline PM 2002 CC model; Planmeca Oy, Helsinki, Finland). The focus median plane distance was 152 cm with standardized exposure of 73 kV, 15 mA for 0.64 s, and the radiographic film used was Kodak MXG (18 × 24 cm2; Kodak, Tokyo, Japan). A sheet of transparent acetate was placed over the lateral cephalometric radiographs, and the anatomical structures were outlined. Overjet, overbite, and the following angular measurements - GoGnSN°, FMA°, U1SN°, IMPA°, and UL-L1° - were performed on these radiographs (Figure 2).
Fabrication of retainers
Immediately after the removal of the fixed appliances, alginate impressions were poured to obtain models of the maxillary and mandibular arches. Essix retainers were thermoformed from 0.040-inch sheets (type C) according to the manufacturer's instructions. Hawley retainers that included Adams clasps and molar-to-molar labial bows supported with lingual acrylic were fabricated. The labial bows extended to the posterior region and were soldered to the Adams clasps. The patients were instructed to wear their retainers full-time (except during meals) for a period of 1 year.
Data analysis
The differences between the Essix and Hawley groups were compared using repeated measures analysis of variance (ANOVA) to identify statistically significant differences between time intervals. Changes between T1, T2, T3, and T4 time points within the same group were analyzed using the Bonferroni test. Changes between the 2 groups were compared using the Mann-Whitney U-test. All statistical analyses were performed using the SPSS (version 14.0; SPSS Inc., Chicago, IL, USA). p-values of < 0.05 were considered statistically significant.
To assess measurement precision and reliability, a total of 10 randomly selected maxillary and mandibular dental casts were re-measured, and cephalometric films were retraced and re-measured by the same two examiners at a 2 week interval (i.e., 4, 3, and 3 casts from the pretreatment, post-treatment, and post-retention stages, respectively). The casual error was calculated according to the Dahlberg formula.14 Also, intra-class correlation (Cronbach's alpha) analysis was applied to the same measurements to supplement the results obtained using the Dahlberg formula.
RESULTS
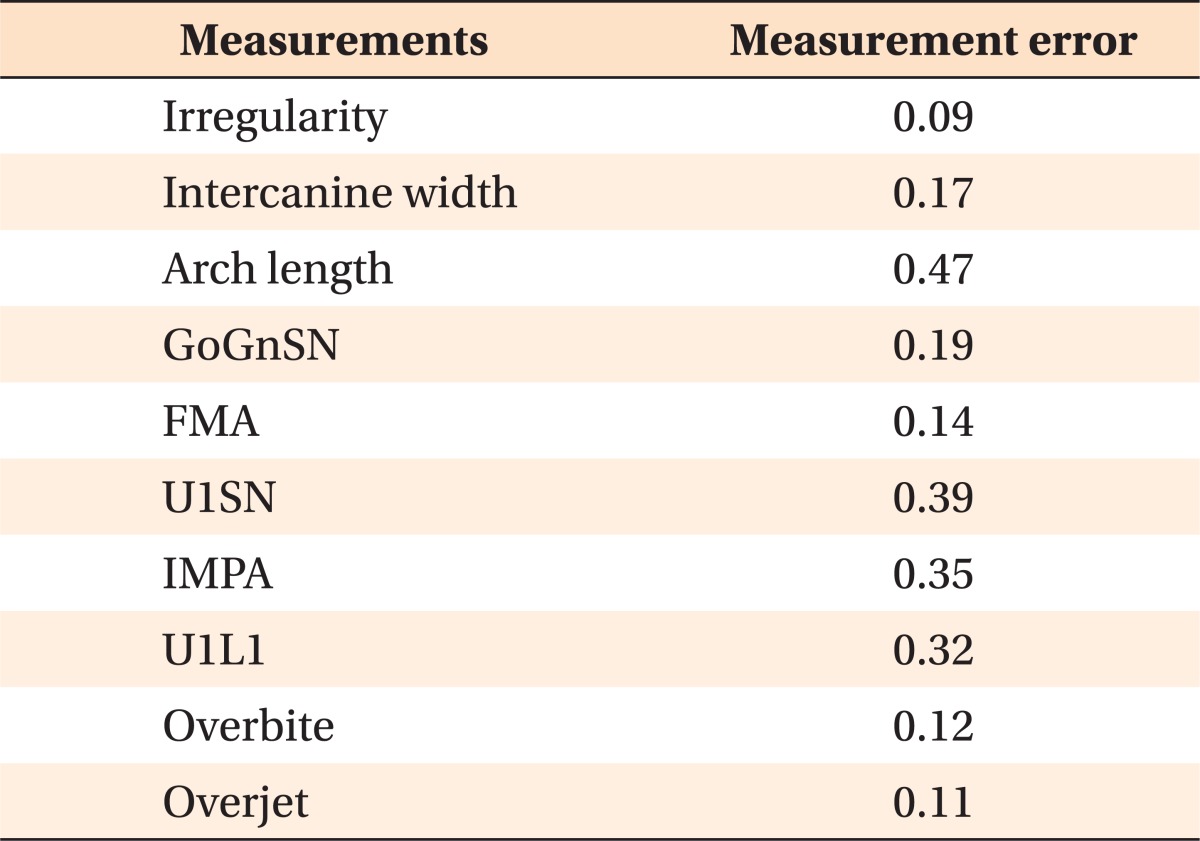
The age and gender distributions between the groups were similar (Table 1). For all parameters measured in this study, Cronbach's alpha was very close to the ideal value of 1 (0.934 - 0.980 for the cephalograms and 0.941 - 0.982 for the impressions). The mean linear measurement error obtained with Dahlberg's formula was between 0.09 and 0.47 mm, and the mean angular measurement error was between 0.14° and 0.39°, which was near the ideal value of zero (Table 2).
Tables 3 and 4 present the means and standard deviations of treatment changes and the degree of relapse at the pretreatment, posttreatment, postretention, and follow-up stages. The irregularity index rebounded slightly from the postretention to the follow-up phase in both groups, but the patients wearing Essix retainers showed slightly more incisor irregularity in both arches than those wearing Hawley retainers at the follow-up stage; however, this difference was not statistically significant (p > 0.05) (Table 3). The mandibular arch length measurements tended to return to their original values in both groups; however, the values were significant only in the Hawley group (F = 6.78). Cephalometric measurements revealed minimal differences between the 2 groups, such as slightly higher protrusion of the upper incisors in the Essix group during orthodontic treatment (Table 4).
DISCUSSION
Retention and subsequent relapse are two of the most important concerns in orthodontic treatment. Retention is not a separate problem or phase in orthodontics, and the type of retention and retainers used should be considered during diagnosis and treatment planning.15-17 To the best of our knowledge, this study is the first to investigate the clinical effectiveness of Essix and Hawley retainers during active retention for 1 year and after a 2-year follow-up period. Previous studies that investigated these appliances were carried out only for a 6-month active retention period.11,12
Lindauer and Shoff11 carried out a prospective study to compare the efficacy of Essix and Hawley retainers. They modified the design of the Essix retainer and covered only canines and incisors that might cause posterior extrusion and anterior open bite. In their study, the researchers focused on overbite, overjet, and irregularity index and compared the changes over a 6-month retention period; they found no significant differences between the 2 retainers.
Rowland et al.12 compared the effectiveness of Hawley and vacuum-formed retainers in a randomized study with a large sample size carried out over a 6-month retention period. There were numerous instances of malocclusion and treatments performed. They reported that vacuum-formed retainers were more effective in the lower incisor region.
In another randomized study, Barlin et al.18 investigated the effectiveness of Hawley and vacuum-formed retainers in maintaining incisor irregularity, intercanine and intermolar widths, and arch length. While they reported a degree of relapse during retention, there was no statistically significant difference between the effectiveness of the 2 types of retainers.
While orthodontists are sensitive to changes in tooth positions, from an aesthetic standpoint, relapse of the anterior teeth alone weighs heavily in any assessment of the stability of a treatment result because patients are exclusively perceptive to the alignment of their incisors and canines. Many studies focused on the changes at the anterior segment after orthodontic treatment, especially in the mandible. In our study, anterior crowding was evaluated with Little's irregularity index, which was also used in the maxilla, similar to the study by Taner et al.19
When we examined the changes in the mandibular irregularity index from the post-treatment to the postretention periods, the Hawley group showed a significant difference between the 2 periods (F = 23, 15; T2 - T3, T4), whereas there was no significant increase in the Essix group (Table 3). Therefore, we found Essix retainers to be more effective than Hawley retainers in the mandible. This result confirms the results obtained by Rowland et al.,12 but they are not compatible with those obtained by Barlin et al.,18 who found no difference between the Hawley and vacuum-formed retainers in both arches. The degree of relapse was clinically more significant in the mandibular arch than in the maxillary arch, thus confirming the results obtained by Rowland et al.12 We concluded that both retainers were successful (p > 0.05). However, the Essix appliances were more efficient in retaining the anterior teeth in the mandible (Table 3). Irregularity of the incisors, particularly in the mandible, commonly develops after retention.20-22
There were no statistically significant differences between the effectiveness of the Essix and Hawley retainers with regard to retaining intercanine arch width in both arches. Our results are supported by the findings of Rowland et al.12 Similarly, there was no statistically significant difference in changes in the intercanine arch width during the follow-up period, which might have been considered as relapse.
Previous studies concluded that increases in the dental arch length during orthodontic treatment tended to return to the pretreatment values after retention. Our findings are in agreement with those of previous studies.21-24 The mandibular arch lengths increased during treatment and tended to return to their original values after retention in both groups; however, these changes were statistically significant only in the Hawley group (F = 6.78; T4 - T2, T3). This increase in the mandibular arch length was maintained to a greater extent in the Hawley group than in the Essix group during retention (p > 0.05). However, the mandibular arch lengths returned to their pretreatment values after retention in both groups. Similarly, the maxillary arch lengths also increased during treatment and tended to return to their original values after retention in both groups.
Although there is no universal agreement concerning retention protocols for removable appliances, many authors have advised that these appliances should be worn for at least 1 year after orthodontic treatment.4,5,25,26 The treatment origin for malocclusion and the treatment modalities used are other factors that affect stability following orthodontic treatment. The patients recruited in our study were selected from patients with anterior crowding with skeletal class I and angle class I malocclusions or skeletal class I and slight angle class II malocclusions. All the patients were treated with fixed appliances without extractions, and interproximal stripping was carried out when needed. The patients' age and gender distribution between the Essix and Hawley groups did not show any significant difference (Table 1).
Many factors affect the stability of teeth following orthodontic treatment, such as posttreatment facial growth and development and forces from periodontal tissues, orofacial soft tissues, occlusal factors, and occlusal forces.25 The effect of the type of retention device on tooth stability is still controversial. Previous studies have compared the characteristics of these appliances, but not the changes during the follow-up period after the appliance is removed.
Al Yami et al.27 evaluated dental casts of 1,016 patients for long-term treatment outcome. They concluded that about half of the total relapse occurs during the first 2 years after retention. A 2-year follow-up is an insufficient period to compare the degree of relapse in these 2 groups; however, the results of our study will provide a preliminary opinion about the retention characteristics of Essix retainers.
During the retention period, patients were called after a 6-month interval. Three patients from the Hawley group and 1 patient from the Essix group were excluded from the study because they did not wear their retention appliances during this period. According to our observations, the patients from the Essix group were more cooperative than patients from the Hawley group.
After a 2-year postretention period, the mandibular irregularity index increased in both arches in both groups (F = 30.87 and F = 23.15 in the Essix and Hawley groups, respectively). The degree of relapse was slightly higher in the Essix group, which might have been due to the higher initial values (p > 0.05). Similarly, the initial dental and cephalometric variables did not show significant differences between the groups (Tables 3 and 4).
In the cephalometric analysis, there were some differences between the 2 groups in the U1SN°, U1L1°, and overbite measurements (Table 4). The origin of this difference was the higher upper incisor protrusion values in the Essix group after treatment. The U1SN° was slightly reduced in both groups with maxillary irregularity index. The IMPA° was slightly increased in the Essix group but decreased in the Hawley group. These results were similar to those of previous studies that indicated no significant correlation between the long-term stability of the mandibular anterior teeth and any of the cephalometric measurements.22-24,28
Bonded retainers were considered more effective in maintaining incisor position, especially in the mandibular arch. However, the Cochrane review by Littlewood et al.29 and the study by Atack et al.30 concluded that there is no reliable evidence indicating that bonded retainers are more effective than vacuum-formed retainers.
Clinicians should be aware of the relapse potential of malocclusions, especially crowding. They must inform their patients before treatment that relapse may occur as a result of natural adaptation after removal of the appliances. Both Hawley and Essix retainers are preferred for use as removable retention appliances. Other factors such as cost, patient preference, cooperation, satisfaction, and occlusal contact patterns might influence the choice of retainer. Further clinical studies with larger randomized samples are necessary to investigate the relation between these appliances.
CONCLUSION
Our study revealed that the retention characteristics of both Essix and Hawley retainers are similar. The Essix retainers were found to be more effective in maintaining mandibular incisor positions during retention. However, all variables tended to return to their original values 2 years postretention, regardless of the retainer type.
 XML Download
XML Download