

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The limitations of traditional tooth movement have been overcome by orthodontic mini-screws,1-6 and mini-screws are now increasingly applied in dentistry. Orthodontic mini-screws are used to improve orthodontic treatment efficiency and have been gaining popularity because of their simple insertion procedure and non-requirement of patient cooperation. However, use of mini-screws does not always guarantee treatment success, and stability of the mini-screw is essential for promoting anchorage. Orthodontic mini-screws are mostly inserted by the self-drilling method using hand drivers.7,8 Various articles on orthodontic mini-screw placement have reported the use of motor-driven handpieces. Mini-screws can be inserted using endodontic contra-angle or surgical implant motors and handpieces.1-3 Surgical implant motors play a pivotal role in the placement of prosthetic implants. Root canal treatment can be safely performed using an endodontic motor. Endodontic motors can maintain rotational speed, control torque, and reduce the risk of NiTi file breakage.9 The rotational speed control and high torque setting of surgical implant motors provide sufficient power for penetrating the alveolar bone. The endodontic contra-angle handpieces can be connected to low-speed motors of the dental unit for drilling the alveolar bone. However, air motors of the dental unit may not provide sufficiently high torque to drill the alveolar bone.1,3
Motor-driven handpieces can stabilize the orientation or angle of the drilling, decrease the risk of mini-screw fracture at the apex by preventing excessive pressure during self-drilling, and maintain a constant drilling speed. However, motor-driven instruments are expensive and require presetting of the motor before the insertion procedure.2
Insertion of mini-screws with the hand driver by an inexperienced orthodontist may cause the mini-screws to wobble or wiggle out of place, and stability can be compromised. Furthermore, it is difficult to maintain the appropriate rotational speed or torque, and access to the palate or the right or left side of the intraoral target areas can be limited with the hand driver.10-14 Failure of mini-screw placement can lead to prolonged treatment duration. The risk of adjacent root damage can also be increased if larger diameter mini-screws are inserted in previously failed mini-screw sites. If a mini-screw of the same diameter is placed at the failed mini-screw site, an alveolar bonehealing period of 2 - 3 months is required.4
In the literature factors that affect the stability of the mini-screw still remain controversial. According to previous studies, the potential factors that affect stability include age, gender, insertion site, screw length, screw type, onset and method of force application, soft tissue management, placement side, tissue type, and oral hygiene.15-20 These studies evaluated the effects of gender, age, length, and location of mini-screws inserted using a hand driver only. Therefore, in this study, we evaluated the effects of different insertion methods on the success rate of mini-screw placement. In this investigation we aimed to compare the success rates of the motor-driven insertion method with that of the conventional manual insertion method using a hand driver.
MATERIALS AND METHODS
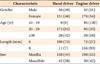
Two hundred eighty-six patients (73 men, 213 women) received 429 orthodontic mini-screws (102 in men and 327 in women) (Dualtop, Jeil Medical Co., Seoul, Korea); of these, 262 mini-screws were 6 mm in length and 1.6 mm in diameter and the remaining 167 mini-screws were 8 mm in length and 1.6 mm in diameter. Three hundred fifty-seven mini-screws were placed in the maxilla and 72 were inserted in the mandible. Ninety-five mini-screws were placed in patients in their 10s, 268 mini-screws in patients between 20s, and 66 mini-screws in patients in their 30s or older (Table 1).
The motor-driven insertion method was used for inserting 228 mini-screws, and the conventional manual method was used for the remaining 201 mini-screws. The manual insertion method was used at our clinic between 2005 and 2009 while the 228 motor-driven mini-screw placements described in this study were inserted after 2009 until 2010. Mini-screws that showed any mobility or loosening were assessed as failures at the follow-up examination conducted more than 6 months after insertion. Mini-screws were placed under a torque of 20 N·cm and a rotational speed of 15 rpm.
At the site of mini-screw insertion, a stab incision was carried out with a #15 blade after local infiltration, and mini-screws were subsequently inserted. A newly developed orthodontic motor engine (Orthonia, 111-ED-010, Jeil Medical Co.), which can maintain the torque and a low insertion speed was used for the motor-driven insertion method.3
Statistical analysis
Cross-tabulation analysis was used to compare the success rates between the motor-driven and manual insertion methods based on gender, mini-screw length, age, and site of mini-screw insertion. The Cochran-Mantel-Haenszel test was used to compare the success rates of the 2 insertion methods. The significance level was set at p < 0.05 for all analyses. All statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
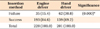
The overall success rate of the motor-driven method (84.6%) was significantly higher than that of the manual insertion method (69.2%; p < 0.001) (Table 2).
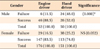
In men, the overall success rate of mini-screw insertion was 70.6% and significantly higher success rates were observed with the motor-driven method (88.5%) than with the hand driver (52.0%; p < 0.001). In women, the overall success rate was 79.5%, and no significant difference was found between the success rates of the motor driver and hand driver (83.5% and 74.8%, respectively) (Table 3).
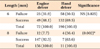
With respect to mini-screw length, the overall success rate of the 6-mm-long mini-screws was 69.1%, and it was not affected by the insertion method. The overall success rate of the 8-mm-long mini-screws was higher (90.4%) than that of the 6-mm-long mini-screw. Moreover, the success rates of the 8-mm-long mini-screws were significantly higher with the engine driver than with the hand driver (92.3% vs. 63.6%, p < 0.01) (Table 4).
Regarding the insertion site, the overall success rate of insertion in the mandible was 61.1%, and the success rate of the engine driver was significantly higher than that of hand driver (80.0% vs. 47.6%; p < 0.01). The overall success rate of insertion in the maxilla was 80.7%, and the success rate of the engine driver was also significantly higher than that of hand driver (85.4% vs. 74.8%; p < 0.05) (Table 5).
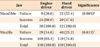
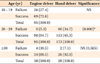
Concerning age, mini-screws were placed only using the engine driver for patients under 20 year of age. The overall success rate in these patients was 72.6%. For patients in their 20s, the overall success rate was 75.7%. In these patients, significantly higher success rates were obtained with the engine driver than with the hand driver (94.7% vs. 65.3%; p < 0.001). For patients older than 30 years of age, success rates were not affected by the insertion method (89.5% for the engine driver, 92.9% for the hand driver). Among all the age groups, the highest success rate (90.9%) was observed in the group older than 30 years of age (Table 6).
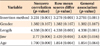
The Cochran-Mantel-Haenszel test revealed that the insertion method, screw length, and site of insertion were statistically significant variables that affected the success rates of mini-screws (Table 7). Improvement in success rate was also more pronounced with the engine driver than with the hand driver.
DISCUSSION
In this study the success rates of manually inserted mini-screws using the hand driver were compared with those of motor-driven mini-screws using the orthodontic engine driver. We found that the engine driver insertion method, screw length, and site of insertion significantly affected the success rate of mini-screw placement. Furthermore, the engine driver method was found to be a predictive factor of higher success rates of mini-screw placement.
Several studies have reported no relationship between the mini-screw success rates and gender or age5,6,14; however, in this study, the motor-driven method was found to yield higher success rates in men than the conventional manual method. Furthermore, the possibility of wobbling during the early stage of screw insertion is higher in men than in women due to the higher bone density in men; this may be reason that the engine driver method, which exerts less insertion force during the initial stage, yields higher success rates than does the conventional method. Lim et al.21 reported similar results in his study and postulated that the stronger occlusal force in men contributed to this finding.
When the engine driver was used, the 8-mm-long mini-screws exhibited higher success rates than the 6-mm-long mini-screws. Similarly, Chen et al.5 reported higher success rates with the 8-mm-long mini-screws than with the 6-mm-long mini-screws, and stated that mini-screw length was one of the factors affecting successful placement.
With respect to the site of mini-screw placement, in this study, the maxilla was associated with overall higher success rates of mini-screw placement than was the mandible. Although the engine driver exhibited improved success rates in both the maxilla and mandible, the amount of improvement in success rates by using the engine driver was higher in the mandible. As mentioned earlier, the higher cortical bone density of the mandible in men tended to cause increased wobbling during the initial stage of placement. Therefore, the higher success rate may be attributed to the lower insertion force exerted by the motor-driven driver, resulting in decreased wobbling.
Regarding age, an appropriate assessment could not be performed for patients older than 40 years of age because of the insufficient sample size, and for patients under 20s, because mini-screws were not usually placed for them. However, various studies report that the success rates of mini-screws is independent of age.22
In 2010, Crismani et al.23 reviewed 14 published clinical trials5,12,17,18,24-32 on the success of mini-screw placement and found that the average success rate was 83.6%. According to our study, the success rate increased from 69.2% with a hand driver to 84.6% with an engine driver. However, the success rate was not significantly higher compared to that reported in previous studies. This may be related to differences in individual orthodontist's skills.
We used cylinder-type mini-screws (Dualtop, Jeil Medical Co.) in this study. According to the study by Lim et al.,33 the drilling time required for cylinder-type mini-screws is longer than required for the tapered-type mini-screws, especially during penetrating the cortical bone when the drilling torque was continuously measured from the initial stage of placement. Therefore, the engine driver is expected to decrease wobbling after initial penetration of the screws especially when using cylinder-type mini-screws.
When inserting mini-screws using the hand driver, stability of the mini-screw head is compromised by torsional stress due to wiggling.34 In contrast, the engine driver provides adequate torque and power, and maintains a constant speed during drilling. The engine driver is also safer due to the auto-stop mechanism (over-limit mechanism) when greater than the designated insertion force is applied to place the mini-screw into the alveolar bone.35,36 For an inexperienced orthodontist, the engine driver can be helpful in improving success rates of mini-screw placement because it has been known to provide better outcomes to beginners in some cases.2 The engine driver is also useful for stabilizing the orientation of insertion into the palate or the most posterior area of the mouth during mini-screw placement. However, the hand driver provides better tactile sensation and awareness with respect to insertion angle and force for beginners. Therefore, for improving clinical skills, the hand driver is recommended for beginners; they can move on to the engine driver once they are sufficiently trained for verifying tactile sensations.
Although the surgical implant engine or endodontic rotary engine can be used, an implant engine is expensive, takes up considerable space, and its settings cannot be easily changed. Furthermore, endodontic engines or reduction handpieces may not provide sufficient torque or power. Therefore, the engine driver, designed specifically for insertion of orthodontic mini-screws, is a feasible alternative solution.
The application of excessive pressure during mini-screw placement can lead to the failure of mini-screws due to excessive tension in the alveolar bone. Tactile sensation can be lost due to high pressure, and insertion orientation can become less ideal. When excessive torque moment is applied during insertion, a screw can be fractured. Therefore, a maximum torque moment of 20 - 40 N·cm is applied, depending on the mini-screw systems and manufacturers.4 In this study, a torque moment of 20 N·cm was applied.
When using the engine driver, an orthodontist should ensure that the engine is fully recharged and the shaft is securely connected to the driver holder. Novice orthodontists need to understand that the tactile sensation of the engine driver differs from that of the hand driver when the mini-screw tip encounters the alveolar bone.37 Matsuoka et al.38 reported that the installation of self-drilling screws at high speeds was not recommended. They recommended using low speeds of less than 150 rpm. When placing mini-screws with a diameter of 1.6 mm at an insertion speed of less than 150 rpm, no bone damage-inducing temperature increase was found to occur.
Thus, the engine driver is recommended in order to maintain low insertion force and low speed,2 because excessive force can induce slippage regardless of bone density. In this study, mini-screws were inserted using an engine driver at an insertion speed of less than 15 rpm to minimize screw slippage and bone overheating.
Thus far, specific protocols regarding torque and force have not yet been established for different sites such as the palate and buccal alveolar bone of maxilla and mandible. Although a few studies have recommended that insertion be performed at a torque of 5 - 10 N·cm,24 further studies are warranted to confirm this.
Luzi et al.15 reported that inaccurate insertion methods were the primary cause of mini-screw insertion failure. Other contributing factors included insufficient irrigation, increased drilling speed, wiggling movement of the driver, and inappropriate insertion torque. They suggested that an orthodontist's experience is the most important factor affecting the success rate of mini-screw placement.
A limitation of this study might be the skill of the orthodontist who performed all the procedures. The same orthodontist performed mini-screw placement by hand driver until 2009 and motor-driven insertions since 2009. It can be argued that his skills improved over time and may have contributed to the improved success rates of mini-screw placement with the engine driver. However, it must be noted that the orthodontist already had 7 years of experience with mini-screw placement in the year 2005. Due to the nature of this retrospective study, it was not possible to adjust for the varying skill levels of the surgeon according to experience.
Furthermore, the only insertion sites assessed in this study were the maxilla and mandible. Further studies are required to evaluate the success rate of the motor-driven insertion method for mini-screw placement at other insertion sites, and to verify the reduction in the gap at the implant-bone interface due to reduced wobbling attributed to the use of an engine driver.39,40
CONCLUSION
In this study, the success rates of manually inserted mini-screws using the hand driver were compared with those of motor-driven mini-screws using the orthodontic engine driver. The main findings of this study are as follows.
The overall success rate was higher when the engine driver was used. When the engine driver was used, 8-mm-long mini-screws exhibited higher success rates.
Regarding gender, success rates were significantly higher in men when the engine driver was used. In women no statistically significant difference, with respect to insertion method, was found.
Regarding insertion sites, higher success rates were observed in the maxilla than in the mandible. Although the engine driver improved the success rate of mini-screw placement in both the maxilla and the mandible, the amount of improvement in success rates by using the engine driver was significantly higher in the mandible.
In conclusion, the engine driver is one of the helpful tool for improving the initial stability of orthodontic mini-screws.
 XML Download
XML Download