

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Functional constipation (FC) is one of the most common gastrointestinal (GI) problems in children with prevalence rates ranging from 0.7–29.6% world-wide [1]. The large variation is due to differences in study methodologies and definitions of constipation. In a large Korean study among secondary or tertiary care hospitals the prevalence rates ranged from 1.8% to 13.9% [2]. According to a study from the United States, the prevalence and burden of childhood constipation has continued to increase over time [3]. Various studies reported chronic constipation has a considerable impact on children's well-being and is correlated with impairment on their quality of life [45].
In order to determine the most effective treatment methods for reaching successful outcomes along with the prevention of relapse, an understanding of the natural course, as well as the prognostic factors of this disease, is necessary. Although there are several drugs in the maintenance phase for the treatment of constipation, osmotic laxatives are accepted as the first treatment option. Lactulose, a synthetic disaccharide, and milk of magnesia (MOM), a suspension of magnesium hydroxide in water, are two osmotic laxatives that have been widely used in Thai children for several years. Recently, polyethylene glycol (PEG) has been introduced as a new and effective drug in both disimpaction and maintenance phases. It is a biologically inert, water-soluble polymer that is minimally absorbed in the GI tract and not metabolized by colonic bacteria. It has not only an osmotic effect but also has an ability to form a unique interaction with water molecules, which leads to an increase in the water content of the stools [6]. Therefore, PEG has been recommended from the European Society for Paediatric Gastroenterology Hepatology and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition to be the first line treatment because it results in greater stool frequency, less additional laxative therapies, and less adverse effects compared with lactulose or MOM [78].
For low-middle income countries, PEG is expensive and not as readily available as MOM and lactulose. Therefore, MOM and lactulose (usage in children <1 year old) has been used for first line treatment for a considerable period of time. To our knowledge, there are limited studies comparing the efficacy of MOM and PEG in real practice. This may be due to several reasons such as low socioeconomic status, poor compliance to treatment, and high rate of lost to follow-up.
Moreover, many studies [91011121314] investigating prognostic factors for treatment outcomes have reported varied results. A recent systematic review [15] included a number of studies with different populations and different study methodologies with conflicting results. It is therefore difficult to conclude which factors are actually predictive for treatment outcomes.
The aims of this study were to evaluate and compare clinical features as well as the clinical course of FC in children aged ≤15 years treated with different medications and to identify prognostic factors related to treatment outcomes, specifically recovery from constipation and relapse.
MATERIALS AND METHODS
We performed a structured, medical record review of patients aged ≤15 years who were diagnosed with FC according to the Rome IV criteria [16] between January 2007 and December 2015 at the GI clinic, Songklanagarind Hospital. Patients who were followed up for less than 6 months or were found to have any organic GI diseases or neurological problems were excluded from the study. The study was approved by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University (IRB no. 59-107-01-1).
Variables collected from the medical records included demographic characteristics, clinical manifestations, dietary history, family history of constipation, investigations, medications given, and outcomes. Improvement was defined as a presence of bowel movement ≥3 times per week together with an absence of hard stool and diagnosed symptoms, which included soiling, painful defecation, and withholding symptoms. Recovery was defined as improvement without the use of laxatives. Persistent constipation was defined when patients' symptoms did not improve. A relapse was defined as a period of at least 2 weeks of increasing symptoms where laxatives had to be reintroduced after a period of medication stoppage. A positive history of cow's milk protein allergy (CMPA) was defined as the presence of symptoms after exposure to cow's milk together with a presence of cow's milk protein-specific immunoglobulin E and/or a positive skin prick test to cow's milk and/or improvement of presented symptoms after cow's milk elimination [17].
All data were analyzed using R language and environment [18]. Statistical significance was defined as p<0.05. Categorical data were analyzed using Fisher's exact and χ2 tests. All continuous variables were reported as median with range or interquartile range, and mean with standard deviation as appropriate and compared using the Wilcoxon test or Student's t-test as appropriate. The frequency and timing of first recovery and relapse were presented in Kaplan Meier curves without adjustment for the discrete nature of the follow-up. Significant prognostic factors for time until first recovery and time until relapse were determined using Cox proportional hazards regression models. The strength of association is presented using hazard ratios and 95% confidence intervals. Patients were divided into 3 groups according to age; infant and toddler (≤3 years), preschool age (3–6 years), and school age (>6 years) in order to evaluate factors associated with treatment outcome.
RESULTS
During the 8-year study period 104 patients (55 male, 52.9%) were identified and diagnosed with FC based on the Rome IV criteria and followed up for a total of 825 visits. The median age at diagnosis was 2.8 years (range, 0.4–11.9 years), age of onset was 1.5 years (range, 0.2–11.3 years) and the median duration from symptoms onset to diagnosis at the GI clinic was 12.8 months (range, 0.3–105.8 months). Most patients were diagnosed during their infancy and toddler period (<3 years; 53%), but the symptoms occurred within the first year of life in 32% of patients. The median follow up duration at the clinic was 18.0 months (range, 6.0–84.2 months). The median number of follow up visits per patient was 5 (range, 1–35) with the median interval between visits being 86.9±118.4 days.
Overall, 22 patients had PEG without electrolyte (PEG4000®; Forlax, Ipsen, France) for the maintenance phase of treatment; only 7 patients were prescribed PEG at the first visit, while the others were switched from another medication during their follow up visits. The median age at diagnosis and age of onset were not different between patients who received PEG (PEG group) and those who did not (non-PEG group). However, the duration of symptom to diagnosis in the PEG group was significantly longer than that of the non-PEG group (p=0.048) (Table 1). In contrast, the duration of treatment before visiting the GI clinic and duration between each follow up visit in the non-PEG group were significantly longer than that of the PEG group. Moreover, patients in the PEG group reported fecal impaction at initial diagnosis more so than those in the non-PEG group.
History and investigations
At diagnosis, all patients fulfilled the Rome IV criteria for FC with the most common symptoms being hard stool (94.1%), withholding symptom (85.3%), lower defecation frequency (76.7%), and painful defecation (76.8%). Amongst 72 patients who had causes of withholding symptoms, 89% experienced painful defecation, and 6% each reported a rushed lifestyle and avoidance of defecation at school as the causes of withholding. Approximately 18% had at least one of the ‘red flags’ in their history, which included a delay in passing of meconium (<48 hours), constipation before 6 months of age, and a failure to thrive. Among these patients, organic causes, especially Hirschsprung disease, were excluded by laboratory investigations and all of them had clinical improvement with laxatives at least once throughout the period of follow-up.
Investigations conducted before diagnosis included abdominal X-rays (22%), barium enema (14%), serum electrolyte (13%), thyroid function testing (7%), and anorectal manometry (2%). Abnormal laboratory findings included fecal impaction (n=22), metabolic acidosis (n=9), and absence of rectoanal inhibitory reflex (n=1). However, there was no significant difference in the medical histories and investigations between the PEG and non-PEG groups.
Medications and outcomes
Nearly one-third (27%) required disimpaction at initial presentation to the clinic and the commonly used method was a rectal enema (68%). The method for disimpaction was not different between the PEG and non-PEG groups (Table 2). Most patients (90%) were prescribed MOM as the first-line drug for the maintenance phase, while PEG was prescribed in only 7% of patients. Three patients required two drugs at first visit; MOM with lactulose (n=2) and MOM with bisacodyl (n=1). Among 22 patients who changed their medication during follow up, 15 did not receive PEG at their first visit and changed to PEG at their follow up period. However, none of the patient who received PEG at the first visit changed their medication.
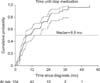
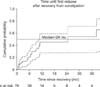
Approximately 76% of patients recovered with a median time to recovery of 9.8 months (Fig. 1). At 1 year follow up, 54% of the patients had successful outcomes after stopping medication. This percentage increased to 78% if asymptomatic patients still receiving medication were included. There was no significant difference in time until first recovery between the PEG and non-PEG groups (p=0.99) (Fig. 2). Among those who recovered, 33% relapsed with a median time until relapse of 24 months (range, 0.5–77.8) (Fig. 3). Treatment outcomes at the last visit and time until first relapse among patients who recovered were not significantly different between the two PEG groups (p=0.06) (Table 2, Fig. 2).
Factors associated with time until first recovery
The following factors were examined in the multivariate analysis; sex, age of onset, age at diagnosis, duration of symptoms to diagnosis, duration of treatment before initial presentation to clinic, constipated symptoms, associated symptoms, family history of constipation, history of CMPA, and history of avoiding school toilets and medications. We found that patients who were >6 years at diagnosis, presented with normal defecation frequency, had no history of CMPA, and had used PEG during the course of treatment were more likely to stop medication at an early time (Table 3).
DISCUSSION
We report clinical characteristics and course of FC in Thai children and found that constipation was commonly diagnosed during the toddler period with a median age of 2.8 years, a result similar to an Italian prospective survey that reported a mean age of onset of defecation disorders to be 2.1±1.8 years [19] as well as a longitudinal study in Amsterdam that reported the median age of onset at 3 years [12]. Di Lorenzo [20] also found the highest incidence of constipation was at the time of toilet training, this being around 2–3 years of age. In this study, approximately one-third of the patients had constipation before the first year of life, which was lower than a previous report [21].
The common drugs used in this study were MOM and PEG, drugs which were different from previously reported longitudinal studies [101112]. van Ginkel et al. [12] and Michaud et al. [10] reported 5- and 10-year-follow up data in children treated withlactulose, respectively. While van den Berg et al. [11] studied children who had constipation before one year of age and found that 53% were given lactulose while 11% were given PEG. Currently, PEG is recommended as first line treatment for FC. It results in greater stool frequency, less requirement for additional laxative therapies, and less adverse effects when compared to lactulose and MOM [78]. Although, previous studies found that MOM is inferior to PEG [822], MOM is commonly prescribed for Thai children in our clinic because of its lower price and ease of accessibility.
A recovery rate of 54% was found at the 1 year follow up period. In previous studies, comparable outcomes were reported; 50% and 59% of children older than 5 years [912] and 59% of those who had constipation before one year of age [11] were considered as reaching a successful outcome without laxatives.
We also found that our recovery rate at 1 year after treatment was close to the rate of successful treatment with or without laxatives in another study in which all patients received PEG as first line therapy [23]. However, our success rate among patients who were still on medication (78%) was slightly lower than that in a study from Amsterdam, which reported a success rate of 83% [12]. This difference might be explained by the difference in medication used, population, and compliance rates.
A recent systematic review [15] also reported a success rate of 60.6%±19.2% after 6 to 12 months follow up in patients who were given laxatives as well as a recovery rate of 49.3%±11.8% in patients who were taken off medication. Comparable to our results, as the time of follow up increased, an increasing number of patients who were successfully treated would be found. However, from the systematic review [15] this finding could only be detected after 5 to 10 years, and the proportion of patients who recover would not increase further.
We could not detect any significant difference of treatment outcomes, especially the time to first recovery, between the PEG and non-PEG groups, a result contrasting with previous studies. A recent randomized double-blind controlled study in 88 Thai constipated children, aged 1–3 years, reported an efficacy of PEG4000® greater than lactulose after four weeks of treatment [24]. Another study in 94 Thai children, aged 1–4 years, found that after four weeks of treatment, children who were randomly prescribed PEG4000® for treatment of constipation achieved 26% treatment success rate more than children in the MOM group [25]. Moreover, a 3-month study in children aged 6 months to 3 years concluded that PEG was significantly more effective than lactulose in terms of appetite, stool consistency, and need for disimpaction [26].
The different results between our study and previous ones may be due to the short duration of follow up in a controlled condition in previous studies. Moreover, our study has a small sample size and results may be confounded by indication. According to general practices in Thailand, most patients will be prescribed MOM or lactulose (children aged <1 year old) as a first line treatment. If the dose of laxatives was increased to the maximum level, without improvement of symptoms, doctors would then change the medication to PEG. As found in our study, only 7% of patients received PEG as first prescription, while only 14% of patients were switched into the PEG group.
The duration from symptoms onset to diagnosis was longer in the PEG group compared to the non-PEG group. The PEG group also needed more frequent follow up visits. Patients treated with PEG might have more severe symptoms, which were more difficult to treat compared to the non-PEG group. Although the treatment outcomes were not significantly different between PEG and non-PEG group, the PEG group probably need more intensive follow up than non-PEG group in order to achieve a similar success rate.
Among those who achieved first recovery, 33% of the patients had a relapse of constipation. Our proportion of relapsed patients was higher than the study of children from Modin et al. [23] and van den Berg et al. [11], which followed up patients for 1 and 3 years, respectively.
In contrast, our rate was lower than the relapse rate in children older than 5 years with an average of a 5 year follow up period [12]. The different relapse frequencies between our study and the one by Modin et al. [23] might be due to the use of different medications-the majority of our patients used MOM, whilst in Modin's study the majority of patients used PEG. However, there might be an effect of selection bias and confounding by indication in our study. This may further have been in realation to most of the patients having been referred to our tertiary center in order for evaluatation of cause, or for the treatment of severe, intractible constipation. We also found that patients in the PEG group had higher relapse rates when compared with those in the non-PEG group (40.9% vs. 20.7%, p=0.09). There were, however, no significant differences between the two groups in terms of time until first relapse. An explantion for this is that the relapsed patients may have swtiched over from other medications to PEG, so as to achieve a more successful outcome. Additionally, it is possible that the duration of follow up may affect differences in relapse frequency. According to Bongers et al. [9], the cumulative relapse rate increased from 28% to 40% after 5 and 7 years of follow up, respectively.
We identified 3 positive factors associated with time until first recovery: age at diagnosis >6 years, normal defecation frequency at diagnosis, and use of PEG during the course of treatment. One negative factor identified was a history of CMPA. Comparably, Bongers et al. [9] also reported defecation frequency as one of the predictive factors to recovery (odds ratio, 1.15). In contrast, there was limited evidence in a systematic review that the ages at diagnosis were not significantly associated with recovery [15]. In our study, age at symptoms onset, duration of symptoms to diagnosis, and duration of treatment before presentation to our clinic were not significantly associated with recovery. Therefore, we suspect that children diagnosed after 6 years of age might have less severe symptoms than that of younger children.
Some studies reported that CMPA was related to childhood constipation [272829]. El-Hodhod et al. [29] also found that CMPA was an etiologic factor for childhood constipation. However, there are limited study reports on the history of CMPA as a predictive factor for recovery.
The strength of our study was that we included children diagnosed with Rome IV criteria and collected data from every follow up visit over a long-term period. We were therefore able to monitor children's symptoms, patterns of prescriptions, and clinical outcomes in real practice, which might be different from a longitudinal prospective study, wherein most children have to adhere strictly to the study protocol and the follow up method using questionnaires. However, some patients' records may have been overlooked using this retrospective method.
In conclusion, we presented a clinical course, a pattern of laxatives used, and clinical outcomes of FC in real long-term follow-up practice. We could not identify any significant difference in treatment outcomes between patients who received PEG and those who did not during the course of treatment.




 XML Download
XML Download