

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Accidental ingestion of a foreign body in children is a relatively common problem, and objects such as ingested batteries mostly pass spontaneously through the gastrointestinal system. But, in about 20% of cases, foreign body ingestion causes complications according to their shape, size or the children's medical status, and thus requiring endoscopic or surgical removal [1]. In particular, button batteries and sharp foreign bodies can be life threatening and difficult to manage by endoscopy. If button cell is retained in the gastrointestinal tract or sharp foreign body is ingested, they can be fatal and most cases require endoscopic retrieval before they move from the stomach to the intestine [2].
To date, there have been no reports on the management of a button battery impacted in the terminal ileum or the colon, having already passed the stomach, and only a few cases have been reported on the endoscopic retrieval of a foreign body in the small intestine or the colon in adults [345].
We report on a case of an ingested disc battery and another case of a sharp foreign body impacted around the ileocecal (IC) valve, separating the small intestine from the colon. Colonoscopic retrieval was successfully performed for both cases.
CASE REPORT
Case 1
A 4-year-old girl was admitted 1hr after unintentional swallowing of a 15-mm-sized disc battery. She was previously healthy and had no other medical history. Her vital signs were stable. Her height was 103 cm (50-75th percentile); weight was 20 kg (90-95th percentile). She did not show signs of nausea, vomiting and abdominal pain. The abdomen was soft and flat with normoactive bowel sounds. There was neither tenderness nor rebound tenderness on the abdomen.
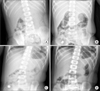
On laboratory examination, only a mild leukocytosis of 11,800/mm3 was revealed. Simple abdominal radiograph showed the radiopaque disc battery in the stomach (Fig. 1A). We anticipated spontaneous passage and decided to follow up with additional serial abdominal radiographs. Those revealed that the battery had migrated from the stomach to the IC valve (Fig. 1B). But, 3 days later, the battery still remained at the IC valve with the follow-up abdominal X-ray picture (Fig. 1C).
Colonoscopic examination on the 3rd admission day revealed that the disc battery still remained stagnant at the same site at the terminal ileum near the IC valve. However, the disc was not accessible due to a large amount of feces in the cecum. After proper bowel preparation using a lavage, colonoscopy was performed again on the 4th admission day. By using a magnet probe attached to the scope, the disc battery was retrieved successfully with minimal mucosal bleeding (Fig. 2). The child was discharged on the following day without any complications (Fig. 1D).
Case 2
A 10-month-old girl had ingested an open safety pin and visited an outside hospital. Abdominal X-ray revealed an open safety pin in the esophagus, and the child was transferred to our medical center for endoscopic removal of the foreign body 6 hours after having swallowed the object. She was previously healthy and had no other medical history. Her vital signs were stable. Her height was 73.4 cm (25-50th percentile); weight was 9 kg (25-50th percentile). She did not show any signs of nausea, vomiting, or abdominal pain. Her abdomen was soft and flat. There was no tenderness or rebound tenderness. Her bowel sounds were normal.
On laboratory examination, only a mild leukocytosis of 20,400/mm3 and mild liver enzyme elevation (46 U/L) was revealed. Simple abdominal radiograph showed a radiopaque 2-cm-sized open safety pin in the stomach (Fig. 3A). We immediately performed an endoscopy but could not find any foreign body in the stomach or the duodenum. We decided to follow up with abdominal radiographs every 6 hour. In the follow up abdominal X-ray, the open safety pin was visible in the lower abdomen (Fig. 3B). The next morning, the open safety pin was located at the right lower abdomen, but serial abdominal radiographs revealed the safety pin had migrated to the IC valve (Fig. 3C). Three days later, the pin still remained in the right lower abdomen near IC valve on serial abdominal X-ray (Fig. 3D).
Colonoscopy was performed on the 4th admission day and revealed the open safety pin stuck in the IC valve (Fig. 4). The pin was then successfully removed by using a tripod forceps and abdominal X-ray after colonoscopy revealed no free air (Fig. 3E). The child remained asymptomatic after colonoscopic retrieval and was discharged without any complications three days later.
DISCUSSION
In pediatric populations, ingestion of foreign bodies frequently occurs. Most ingested foreign bodies naturally pass through the gastrointestinal tract without any clinical sequelae or damage [6]. However, in about 20% of cases, the objects require endoscopic retrieval and 1% of cases may finally require surgical removal. This rate depends on the type of the foreign body, its location, the patient's age, and duration of impaction [78].
Ingestion of button batteries accounts for up to 13% of all foreign body ingestions [9], and it is a special condition, requiring urgent intervention [10]. If the button batteries remain in the gastrointestinal tract, it can cause ulceration, perforation, eventually leading to fistula formation or even death [11]. To date, four mechanisms have been suggested about injury caused by button batteries: leakage of battery contents causing corrosive damage, low voltage burns, pressure necrosis on tissues, and metal toxicity [12].
A button battery impacted in the esophagus needs to be urgently removed, because esophageal injuries can occur within two hours of ingestion, whereas those in the stomach and bowel can be managed conservatively for cases where the patient is presented asymptomatically [13]. However, battery impaction within the intestine or the occurrence of symptoms also requires urgent endoscopic retrieval [7]. Moreover, button batteries with a large diameter (≥20 mm) in children younger than 4 years is more likely to have higher morbidity and mortality [13], whereas most of the small-sized button batteries pass the gastrointestinal tract within 2-6 days [14]. The recent report suggested indication for the observation of ingested foreign body as follows; absence of symptom, children older than 5 years, smaller battery (<20 mm), and short duration of ingestion (<2 hours) [15].
In our case, a button battery with a diameter of 15mm was found in stomach at first presentation and moved to terminal ileum and remained stationary for about 24 hours, but it stayed at the same site for an additional three days without any progress. Even though our patient was 4 years old, an initial observation was decided as she was asymptomatic. However, after confirming the impacted position of the button battery at the IC valve location, colonoscopic retrieval was tried and performed successfully. On colonoscopy, only mild erosion was observed possibly because the disc battery was not so old enough to leak.
Sharp objects are also known as one of the most commonly ingested foreign bodies in children. In a prospective study, 10% of all 244 ingested foreign bodies were identified as sharp objects including straight pins, open safety pins and hairbrush bristles [16]. Ingested sharp objects can cause a variety of complications such as perforation, abscess, peritonitis, fistula formation, appendicitis, aorto-esophageal fistula, and death [17]. If a sharp object is located in the esophagus, it should be removed as soon as possible. Once identified, optimal management depends on the location and type of the foreign body, and the rate of success depends on the skill of the endoscopist and the endoscopic devices such as retrieval forceps, retrieval net, and polypectomy snare [7]. However if the patient is small and weighs less than 5 kg, there would be a limit in using some of the devices [18].
In our case, button battery and open safety pin was both found in the stomach at first presentation and moved to the terminal ileum near IC valve within a day, but they stayed at the same site for an additional three days without any progress. After confirming the impacted button battery and the open safety pin at the IC valve area, colonoscopic retrieval was tried to remove the intestinal foreign body. We could remove the disc battery and the open safety pin successfully using a magnetic probe and a tripod forceps,
respectively, without any complications.
About 1% of ingested foreign body may eventually need surgical removal; however, there have been only a few cases reported on sigmoidoscopic or colonoscopic retrieval of an impacted object at the gastrointestinal tract in adults and children. In case of disc battery, there have been no reports in children to date [345]. If impacted foreign bodies at the gastrointestinal tract be within the scope of endoscopic approaches, colonoscopic removal may be helpful in young children to avoid invasive surgical treatment.



 XML Download
XML Download