

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alimentary tract duplication cysts are rare congenital anomalies which may present anywhere from mouth to anus. However, the most common location being the ileum, followed by jejunum and duodenum [1].
The clinical presentation of duplication cyst varies according to the anatomical location and age of the patient. They may be asymptomatic, incidentally diagnosed or may present with obstruction or volvulus. Here we report a case of a one year old male child presenting with shock and discharging umbilicus. Similar presentation of giant duplication cyst has not been reported in literature till date.
CASE REPORT
A one year old male child presented to the pediatric emergency with history of vomiting, fever, abdominal distension and loose stools for 10 days. There were 6-7 episodes of nonprojectile, nonbilious vomitings. There was no history of blood in the vomitus or in the stools. Fever was upto 38.8℃, intermittent and lasted for 3 days only.
There was a positive past history of loose stools, vomiting and malena 3 months back. His hemoglobin was 3.5 gm/dL for which he received one unit of blood transfusion. As per the parents the mile stones of the baby were normal for his age. The weight of the child was 8 kg, length was 84 cm and occipito-frontal circumference was 44 cm (−2 to −3 standard deviation).
The child presented in a gasping state and required immediate intubation. Glasgow coma scale at admission was Motor response-5, verbal response-intubated, eye opening-3. Pulse and blood pressure were not recordable as child was in state of shock. Abdomen was grossly distended with prominent visible veins with flow of blood away from umbilicus. Liver and spleen could not be palpated due to gross distension. Bilateral flanks were full with positive fluid thrill. Chest and cardiovascular systems were normal. Digital per rectum examination was normal with no blood on the finger.
Child was kept on synchronized intermittent mandatory ventilation mode of ventilation with four ionotropes (dopamine, 20 mcg; dobutamine, 20 mcg; adrenaline, 0.1 mcg; milrinone, 0.5 mcg). He was extubated on day 3 and the ionotropic support was gradually tapered till day 5 of admission.
A provisional diagnosis of severe protein energy malnutrition (PEM) or tubercular abdomen leading to sepsis with multi-organ dysfunction syndrome was kept.
Therapeutic peritoneal tap was done on alternate day (300 mL/tap). Ascitic fluid was transudate with culture showing Acinetobacter, serum-ascites albumin gradient, 1.9 g/dL; adenosine deaminase, 24 IU/L; the child received intravenous imepenem (20 mg/kg every 6 hourly) as per culture and sensitivity. Mantoux test was negative.
An erect abdominal x-ray showed complete ground glass appearance. Ultrasound revealed loculated fluid collection all over the abdomen. All other organs were normal.
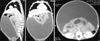
A contrast enhanced computed tomography scan of the abdomen and chest revealed gross ascites (10 Hounsfield unit) with smooth thickening and enhancement of peritoneum. The small bowel loops were clumped and displaced in the center posteriorly because of this tense ascites. A differential diagnosis of mesenteric cyst was also kept (Fig. 1).
The child was on an improving trend and was accepting full feeds normally and passing stools daily till day 9 of admission. On day 10 of admission, there was sudden onset of seropurulent discharge from umbilicus. The decision for exploration was taken because of the massive amount of fluid in peritoneal cavity with purulent discharge per umbilicus.
On exploration the peritoneum cavity had about 1,100 mL of straw colored fluid along with pus. There was a cyst approximately 27×6 cm, communicating with ileum, 10 cm proximal to ileocaecal junction on mesenteric side. The cyst was attached to the umbilicus (just 2 cm proximal to its opening into the ileum) where it got perforated leading to umbilical discharge. This cyst was traversing the mesentery from left to right and then bifurcating into two blind dilated pouch like structures and was spreading between the two layers of the mesentery of ileum for about 30 cm without affecting the vessels (Fig. 2). Cyst was delivered from blind end till its communication with the ileum by opening the mesenteric layers. The communicating part with ileum was narrow, which was cut flushed with ileum and mucosa was stripped off, ileum was closed in 2 layers.
Postoperative recovery was uneventful and the child was discharged on full feeds on day seven. Post-surgery 3 months, the child is doing well and has gained 2 kg.
Histopathology was suggestive of duplication cyst with heterotopic gastric mucosa with multiple papillary projections lined by intact gastric lining epithelium.
Final diagnosis was Duplication cyst of ileum with perforation and discharge from umbilicus.
DISCUSSION
Most duplication cysts manifest during the first 2 years of life with an incidence of 1 in 4,500 by autopsy series, with a slight male predominance [2].
Enteric duplications can be cystic or tubular masses arising from the mesenteric side, unlike Meckel's diverticula. Duplications of midgut or hindgut usually present as acute abdominal distention with or without pain. Heterotopic gastric mucosa may cause ulceration, bleeding or perforation which was noted in index case. Mass effect of the enlarging cyst on the adjacent bowel may cause nausea, vomiting and cramping. A large duplication may be palpable as a mobile mass in up to 50% of patients and may cause volvulus. Presentation may mimic acute appendicitis occasionally. Cyst may act as lead point for intussusception. Stomach duplications may present with gastric outlet obstruction while duodenal duplications usually present with pain and recurrent pancreatitis [345]. Malignant lesions arising from duplication cysts are seen in later decades but are uncommon in children.
The index case is worth reporting as duplication cyst presenting with ascites and PEM with a discharging umbilicus has not been published in the literature till date. A differential diagnosis of infected mesenteric cyst was kept as one possibility but that does not explain malena in this patient. Malena can be seen in patients with Meckel's diverticulum but they do not present with such gross ascites. Hence the diagnosis remained elusive in spite of all investigations till the exploratory laparotomy was performed.
The index case falls into the type II category as per Li et al.'s classification [6] based on vascular supply. Type II lesions are less common (24.6%), but more than 90% of these lesions were associated with thoracic vertebral anomalies, but no associated anomalies were noted in our patient. The knowledge of vascular anatomy of duplications allows for resection of these lesions without resecting the adjacent bowel.
If resection is not possible, one may drain the lesion into Roux-en-Y loop of small intestine or create a large window to adjacent intestine. As there is possibility of ectopic gastric mucosa, it should be removed, either by limited resection or by mucosal stripping [7].
Managing a patient with ascites and shock can be a challenge to the treating physician. Duplication cyst should always be kept as a differential diagnosis, as perforated cyst with massive peritoneal fluid can be misinterpreted as ascites so that early intervention can help in better management.

 XML Download
XML Download