

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Obesity is one of the most common public health problems among children. The worldwide prevalence of childhood obesity has increased in recent decades [12], and the incidence of childhood obesity is also rising in Korea [3].
While the exact reason for this increasing prevalence of obesity is unclear, it is widely believed that genetics [4], ethnicity [5], lower physical activity [6], diet [7], shorter sleep [8], and socioeconomic status (SES) [9] contribute to the etiology of obesity.
SES is a well-known risk factor for childhood obesity, although many controversies remain regarding the association between SES and obesity. Many previous studies have reported that individuals with lower SES are at an increased risk for obesity than those with higher SES [910], but other studies reported that individuals in higher SES groups tend to be more obese than those in low SES groups [1112]. In previous Korean studies [131415], results have shown that SES might be an important risk factor for childhood obesity, but the results have not been consistent. Therefore, we investigated whether lower SES was associated with childhood obesity using the most recent dataset (Korea National Health and Nutrition Examination Survey [KNHANES]: 2010-2012).
MATERIALS AND METHODS
Study population
This study was based on data obtained from the fifth KNHANES. The KNHANES was a cross-sectional survey designed to examine the health and nutritional status of the non-institutionalized Korean population. It was conducted by the Division of Chronic Disease Surveillance at the Korea Centers for Disease Control and Prevention (KCDC). Data were collected in a variety of ways, including household interviews, physical examinations, laboratory tests, and nutritional status assessments. All survey protocols were approved by the KCDC Institutional Review Board. Written informed consent was obtained from all participants before the survey began.
We included 5,250 people younger than 18 years of age from the total of 18,066 who participated in the fifth KNHANES study (2010-2012). We excluded participants who we did not have data from both parents and under 2 years old aged children. The remaining 3,095 participants (1,640 boys and 1,455 girls) were included in the final analysis.
General characteristics, anthropometrics and the definition of obesity
The health interview and health behavior surveys included well-established questions to determine the demographic and socioeconomic characteristics of the participants. These surveys included questions regarding age, sex, height, weight, residence area, family income, education level, employment status, marital status, smoking habits and number of household members. The respondents' residential areas were categorized as urban (an administrative division of a city) or rural (not classified as an administrative division of a city). The definition of a city in Korea is a place where more than 50,000 people live and that is larger than a town. Monthly family income indicates monthly equalized family income and was calculated by dividing total family income by the square root of the number of household members. In KNHANES, monthly family income was classified into quartiles to determine monthly household income level (1, low; 2, middle low; 3, middle high; 4, high). Education level was defined as less than high school, high school or college or more. Cigarette use was divided into three categories: current smoker, ex-smoker and non-smoker.
The directly measured anthropometric data (height, weight and body mass index [BMI]) were transformed to the age- and sex-specific percentiles based on the 2007 Korean Growth Charts [16]. The weight status of children was classified as obese (BMI, ≥95th percentile for BMI-for-age), overweight (BMI, 85th to 95th percentile), and normal weight (BMI, <85th percentile) according to the 2007 Korean National Growth Charts [16]. The weight status of parents was classified as normal weight (BMI, <25.0 kg/m2), overweight (BMI, 25.0-29.9 kg/m2), and obese (BMI, ≥30 kg/m2) according to World Health Organization reference [17].
Statistical analyses
We conducted all statistical analyses using SPSS complex sample procedure because KNHANES data was collected through a representative, stratified, and clustered sampling method. For more accurate statistical comparisons, univariate analysis was conducted to select significant covariates. After selection of significant covariates, we carried out binary logistic regression analysis to identify the relationships between risk factors and the prevalence of obesity. Statistical analysis was conducted using the IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). For all analyses, p-values were two-tailed, and a p-value less than 0.05 was considered statistically significant.
RESULTS
Table 1 summarized clinical characteristics of participants. A total of 3,095 boys and girls from the 2010-2012 periods of the fifth KNHANES were included in this study, and 3,010 mothers and 2,785 fathers were also included. Most of the fathers were employed (95.5%), and the majority of parent had a higher than high school education level (92.7% for mothers, 89.6% for fathers). Current smoking was more prevalent in fathers (44.5%), while mothers were more likely to be non-smokers (91.0%). The mean age of the children was 10.0±4.6, and the proportion of boys was 53.5%. Most enrolled children lived in urban areas (82.1%). The prevalence of childhood obesity was 7.2%, and the proportion of overweight children was 11.1%.
Upon univariate analysis, we did not find any statistically significant differences in the parental employment status, parental education level, parental smoking history, sex, age, monthly family income, number of household members and residence area between children with and without obesity. Compared with the normal weight children, obese children were more prone to have obese mothers (odds ratio [OR], 3.385; 95% confidence interval [CI], 2.233-5.131), obese fathers (OR, 2.308; 95% CI, 1.374-3.876), overweight mothers (OR, 1.978, 95% CI, 1.194-3.275) (Table 2).
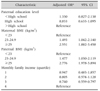
After controlling for confounding factors, the binary logistic regression analysis showed overweight mothers (adjusted OR [aOR], 1.889; 95% CI, 1.079-3.309), obese mothers (aOR, 3.409; 95% CI, 2.228-5.215), obese fathers (aOR, 2.135, 95% CI, 1.257-3.627) were associated with childhood obesity (Table 3).
Overweight mothers (aOR, 1.493; 95% CI 1.042-2.140), obese mothers (aOR, 2.551; 95% CI, 1.882-3.458), overweight fathers (aOR, 1.477; 95% CI, 1.030-2.119) and obese fathers (OR, 2.776; 95% CI, 1.978-3.894), were significant factors in binary logistic regression analysis comparing between children with normal weight and those with overweight and obesity (Table 4).
DISCUSSION
In our study, childhood obesity was positively associated with maternal overweight, maternal obesity, paternal obesity. Parental obesity is a well-known risk factor of childhood obesity [1318]. Our results were similar to results of previous studies. Genetics and environmental components are both known to be associated with obesity. Obesity-related genes are inherited from obese parents to their children [19]. In regard to epigenetics, the inherited obesity-related genes interact with the personal environment and this interaction can drive the development of childhood obesity [20]. Epigenetic changes can influence obesity related hormones such as leptin (reduces food intake and decreases body weight) [21], insulin (increases food intake, adiposity, and peripheral insulin resistance) [22], and ghrelin (promotes feeding, suppresses energy expenditure, and causes weight gain) [23]. Moreover, familial life style is an important risk factor of childhood obesity [24] and parental eating behaviors are likely to determine the dietary patterns of children at an early age [25]. In our study, maternal overweight and obesity more influenced childhood obesity than paternal overweight and obesity. These results were also observed in a previous study [26]. We thought this association due to more similarity in nutrient intake between mothers and children than between fathers and children [27]. Traditionally, in Korea, mothers have more responsibility for children care and takes more time than fathers have.
We did not find any association between parental employment status and childhood obesity. The association between parental employment and childhood obesity was controversial. European study showed maternal work hours have no effect on child overweight and obesity [28], but the other study showed parental work hours increased the prevalence of childhood obesity in United States [29]. We assumed these different results might be due to cultural difference in child care system.
In our study, the association between childhood obesity was not dependent on their age and gender. Because childhood obesity was defined as more than 95th percentile BMI for BMI-for-age in our study, obesity was not significantly associated with gender and age in children.
Our study showed parental smoking was not associated with childhood obesity. The effect of paternal smoking on childhood obesity was inconsistent. Some study reported no association between paternal smoking and childhood obesity [30], but the other study reported positive associations [31]. Previous study showed maternal smoking was positively associated with childhood obesity in non-Hispanic white and non-Hispanic Black mothers, while maternal smoking was not associated with childhood obesity in Asian mothers [32].
We did not find urban-rural differences in childhood obesity. The association between residence area and childhood obesity was controversial. One study reported no difference between residence area in childhood obesity [33], the others study reported higher prevalence of childhood obesity in rural area [34]. Because the proportion of urban residence in our study was higher than previous study [34], we thought higher proportion of residence in urban might have some role in our study result.
In our study, number of household members was not associated with childhood obesity, which was different from a previous study [35]. In a previous study, they reported number of household members was negatively associated with childhood obesity [35]. We assume these results might be due to racial or cultural difference.
Two Korean studies using national representative sample data from KNHANES (2007-2010, 1998-2009) showed that SES did not have any association with childhood obesity [1314]. However, another study using a national representative sample (2009 Korean Survey on the Obesity of Youth and Children) showed that lower SES was associated with childhood obesity [15]. In our study, we found lower SES (parental education, monthly family income) was associated with childhood obesity, but not significant. In previous studies, developed countries have an increasing prevalence of childhood obesity in lower SES group [910], but developing countries showed an increasing prevalence of obesity in higher SES group [1112]. Korea is a recently developed country, and we thought our study results might be similar from other studies in developed countries [910].
This study had several limitations. First, because this study was cross-sectional, we could not confirm causality as an explanation for the observed associations. Second, even though this study was based on a national survey, the different results from previous studies might be due to a selection bias or a recall bias. Despite these limitations, this study has important implications. First, this study used a national, widely sampled dataset to determine the association between SES and obesity in Korean children. Second, we were able to adequately address the association between SES and childhood obesity and to shine more light on the discrepancies in previous Korean studies.
Considering the results of other studies, we suggest that SES might be not an important risk factor of obesity in Korean children. Although this hypothesis will require further study, we conclude that each socioeconomic factor affects childhood obesity in a different manner in each country.



 XML Download
XML Download