

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Human milk is the preferred feeding for all newborn infants and provides all nutrients needed to support growth and development during early life. Human milk contains bioactive components such as prebiotic oligosaccharides and probiotics that have a positive impact on gut microbial colonization, immune maturation and overall health [1,2,3]. Because human-milk feeding is not always possible, infant formula has been developed as a replacement. The maturation of the gastro-intestinal (GI) tract functions is influenced by the dynamic process of the development of the intestinal microbiota, which is considered crucial for a healthy infant [4]. One of the major differences between human milk and cow's milk based infant formula is the almost absence of prebiotic oligosaccharides in cow's milk, resulting in the development of a different GI microbiota, if not supplemented [5]. Breastfed infants typically have a microbiota dominated by bifidobacteria, whereas non-prebiotic supplemented formula-fed infants have a more diverse microbiota [6]. Probiotic bacteria are present in fresh human milk, but absent in unuspplemented infant formula [7]. Fructo-oligosaacharides (FOS), when added to infant formula, have a bifidogenic effect [5,8]. The addition of Bifidobacterium lactis to infant formula results in a normal growth in healthy infants, and a better growth in HIV-positive infants [9,10]. The Committee on Nutrition of the European Society of Paediatrc Gastroenterology, Hepatology and Nutrition (ESPGHAN) reported that the available scientific data suggest that the administration of currently evaluated probiotic- and/or prebiotic-supplemented formula to healthy infants does not raise safety concerns with regard to growth and adverse effects [11]. The safety and clinical effects of one product should not be extrapolated to other products [11].
The safety and tolerance of a new synbiotic infant formula, containing FOS and B. lactis, was evaluated with daily weight gain as primary outcome parameter, and in addition weight-for-length and body mass index (BMI)-for-age z score, length gain, head circumference, and the frequency of functional GI symptoms (regurgitation, defeceation) and crying were monitored.
MATERIALS AND METHODS
Subjects were healthy infants recruited by general paediatricians from i) mothers who had decided to not breastfeed, ii) mother who had decided autonomous to discontinue breastfeeding, iii) mothers who were feeding a different starter formula because they had already choosen to not breastfeed and accepted the switch to the study formula. The participating infants represent an unselected population of healthy infants followed by general paedaitricians.
Inclusion criteria were gestational age between 37 weeks and 42 weeks with a birth weight between 2.5 and 4.5 kg and a postnatal age of less than 3 months. Parents needed to be older than 18 years. Infants were excluded if they were considered to have a congenital condition or any symptoms or manifestations suggesting chronic disease. An approval of the study protocol by the independent Ethical Review Board of the Aristoteleion University of Thesalonica was obtained (IRB no. 347/20-12-2016). Written informed consent was obtained from at least one parent, according to the requirements in Greece.
Eighty general paediatrians from Greece participated in the study. The mean number of included infants per participating doctor was four (range 1 to 12 [min-max]).
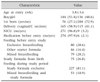
This study was a prospective, open trial over a period of three months intervention with the study formula in 280 infants, whose parents intended to feed their infants (partially) formula and agreed to feed the new synbiotic formula. The characteristics of the infants are listed in Table 1. Parents were informed by the paediatrician about the novel aspects of the study formula. Baseline measurements were collected at inclusion. An appropriate volume for one month of the study formula with written preparation instructions was provided to the parents, who were given the normal recommendations for infant feeding. The study formula was powder infant formula providing complete nutritional support for infants in the first six months of life. The detailed composition, which is in accordance with the Commission Directive 2006/141/EC, is listed in Table 2. Specific for the study formula is the addition of FOS (0.35 g/100 mL) and B. lactis (107 cfu/g powder). Formula was prepared with boiled water which was cooled down to 40℃ at the time of reconstitution. The probiotic is in the formula in an inactive state until reconstitution. After preparation the formula was at body temperature. Infants were fed at libitum. During the three months intervention period infants were either partially breast and study formula fed with a minimal daily intake of 60 mL of the study formula, or fed exclusively with the study formula starting on the day of enrolment during three months. Four visits were scheduled: at inclusion, and after 1, 2, and 3 months. Parents were provided with diaries to record formula acceptance, regurgitation (frequency, volume), defaecation (frequency, composition), crying during the past week. The paediatrician collected the weekly feedback at the end of every month, and filled in the questionnaire according to the information provided by the parents. At each visit, investigators collected anthropometric measures, reviewed compliance (evaluation of the diaries and returned study product) and assessed regurgitation, defaecation and crying according to the information provided in the diaries. Parents were asked to categorize the composition of the stools as liquid, creamy, jelly and hard. Regarding regurgitation, the options for frequency were: absent, occasionally (<1/day), frequent (daily). The options for the regurgitated volume were: no, insignificant or signficiant volume. Regarding crying, data were collected regarding frequency (no, <1/day, daily), timing (day/night), unsoothable crying or not, duration (3 hours or more per day). Pediatricians were asked to score their overall satisfaction of the study formula, on Likert scale 0 (no satisfaction) to 10 (complete satisfaction).
All data were collected and analysed by an independent statistician. The primary outcome was weight gain per day from study entry during 3 months. The secondary outcomes were weight-forlength and BMI-for-age z score, length, head circumference and information on regurgitation, defecation and crying.
At each visit, the weight of each infant was recorded by weighing them twice naked, on calibrated electronic scales, and if deviation was >100 g, an additional measurement was performed. The mean supine length was measuredtwice using a standard measuring board, and in case of a deviation of >5 mm an additional measurement was performed. A non-stretchable slotted insertion tape was used to measure head circumference. In case a third measurement was required, the mean of the two measures closest together was used as outcome.
The weight gain was plotted against the World Health Organization (WHO) Child Growth Standards of breastfed infants. The evolution of the weight-for-length and BMI-for-age z scores were calculated.
Statistical analysis
The weight gain was plotted against the WHO Child Growth Standards of breastfed infants (31). The evolution of the weight-for-length and BMI-for-age z scores were calculated. Changes over study period in continuous variables were evaluated using repeated measures ANOVA. Friedman test was used in case of violation of normality assumption and for ordered variables. Categorical variables were analysed by using chi-square tests (Fisher's exact tests in case that sparse cells occurred) or McNemar's test. All tests were two-sided in α=0.05 level of statistical significance. Statistical analysis was performed using STATA ver. 10 (2007; Stata Co., College Station, TX, USA).
RESULTS
Compliance to the protocol was dependent on the parameters, and ranged from 100% over the three month study period to 45.4% (127/280) due to the collected information on duration of crying at enrolment (Table 3,4,5,6,7). General satisfaction, scored by the pediatricians on a 0-10 score was 9.3 (standard deviation 0.8). There was no infant in whom the study formula had to be stopped and switched to a different formula.
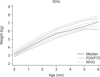
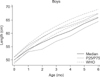
Weight gain of the infants was plotted on the WHO-growth charts for exclusively breast fed infants (Fig. 1 and 2). The median (P50) weight of the girls was at inclusion close to the P50 of the WHO-chart and the evolution over the three month intervention period was parallel to the P50 WHO growth chart (Fig. 1). The median weight of the boys at inclusion was on the P25 of the WHO growth chart, and the evolution was also parallel to the P25 of the WHO chart (Fig. 2). The evolution of the median values of the z scores for weight-for-length and BMI-for-age were at −1 at birth and evolved to 0 after three months of intervention (at the mean age of 3.86±0.82 months) (Fig. 3 and 4). The evolution of weight, length and head circumference was within the expected normal range and is listed in Table 8.
The number of defecations decreased from 22.1 dyring 1 month, over 17.4 during 2 months, to 14.0 during 3 months (Table 5). The number of “hard” defecations was very low as it varied between 2% and 3%.
Regurgitation occurred in 63% of all infants after one month being fed with the study formula, thus at a mean age of almost two months, decreasing to 41.6 % at the age of three months and 20% at the age of four months. Daily regurgitation decreased from 10.9% (1 month intervention) over 3.0% (2 months intervention) to 0.7% (3 months intervention). Only very few infants (−1%) regurgitated significant volumes (p<0.001).
After one month intervention, 15.6% of the infants presented daily crying episodes, decreasing to 3.7 and 0.7 after 2 and 3 months intervention (all p<0.001). Nighttime crying decreased from 38 to 4 % during the three months intervention. The percent of infants with unsoothable crying after one month intervention (median age 1.89 month) was 26.3% of the babies that cried, but only 16% of the total number of infants with information available on crying incidence. After two and three months intervention, the incidence of unsoothable crying decreased to 5 and 0.01%, respectively (median postnatal age 3.89 and 4.89 months) (p<0.001). The percent of infants that cried for three hours or more decreased from 10.5% after one month to 2.2% after two months. No infant cried during three hours or more after three months intervention (mean calendar age 4.89 months) (p<0.001). No serious adverse event related to the study product was reported.
DISCUSSION
The synbiotic formula was well tolerated by all infants, as the test formula was continued in all 280 infants for the three months study period. Overall satisfaction of the paediatricians was excellent, as they scored a median satisfaction of 9.3 on a 10 point Likert scale. For comparison, parents scored 9.0 in a trial with a new femented infant formula supple mented with prebiotics [12]
The primary outcome of the study was the demonstration of equivalence in infant weight gain per day during the intervention according to the WHO growth charts for exclusively breastfed infants. Weight gain was plotted against the WHO growth curves during the first six months of life; the first three months were with the study formula, from the age of 3-4 months up to the age of 6 months infants were fed a diferent starter formula. The curve for girls shows a median value just below the P50 at birth, with an evolution of the median value just below P50 up to the age of 6 months. The curve for boys, however, is different. The median birthweight for the boys was on the P25 of the WHO growth charts, indicating that these boys were relatively small-for-gestational age at birth. At the age of three months, the median weight of the bos is just below the P25 of the WHO-growth chart to end a 6 month just above the P25 WHO-growth chart. However, weight-for-length and BMI-for-age z score for the whole group were low (−1) at birth but evolved towards 0 during the three months study period, suggesting that physical growth and development with the study formula is within the norm.
The number of defecations decreased over the study period. With increasing age, infants produced fewer stools of greater firmness [13]. Infant and follow-on formulas containing B. lactis and galacto-oligoaccharides (GOS) and FOS were reported to be safe, without any additional benefit of the prebiotic over the probiotic [14]. A meta-analysis of seven different trials with infant formula supplemented with B. lactis results in growth similar to what is found in infants fed unsupplemented formula [9]. There is evidence that addition of prebiotics to infant formula alters the GI microbiota resembling that of breastfed infants [15]. Oligosaccharides are added to infant formula because of their presence in breast milk [15].
The Committee of Nutrition of the ESPGHAN reported that according to a systematic review of existing literature, the addicition of B. lactis to infant formula results in a reduction of 46% of the risk to develop acute gastroenteritis [11]. Infants consuming formula supplemented with B. lactis have an increased sIgA concentration in their stools [16]. Furthermore, cesarean-delivered infants consuming B. lactis had a better immune response, as evidenced by increased anti-rotavirus- and anti-poliovirus-specific IgA following immunization [16]. The results of the study by Holscher et al. [16] demonstrate that negative immune-related effects of not breastfeeding and cesarean delivery can be mitigated by including B. lactis in infant formula, thereby providing infants a safe, dietary, immune-modulating bacterial introduction. According to the results of one trial, the administration of Lactobacillus reuteri resulted in a decreased incidence of infant regurgitation, constipation and colic [17].
According to literature, the incidence of constipation is formula fed infants is 7.8% (P25-75: 3.8-15.0%) [18]. Only 3.2% of the infants fed with the new synbiotic formula were reported to have hard stools. Prebiotics are known to result in softer stools than unsupplemented formula, bringing the composition of stools of prebiotic infant formula closer to that of breastfed infants. This effect has been reported for infant formula supplementend with GOS and FOS [19], but also for low levels (0.24 g/100 mL) of GOS [20]. Infant formula supplemented with FOS (0.4 g/dL or 0.8 g/dL) or GOS/FOS (0.8 g/dL) were all reported to induce softer stools [21]. This study reports a similar effect with FOS on stool composition. sIgA in stools is increased in prebiotic supplemented infant formula compared to standard formula [22].
The incidence of infant regurgitation was reported to be 26.7% (P25-75: 14.9-40.9%) [17]. We report an incidence of only 10.9% of infants with daily regurgitation, and only 1.6% in whom the volume was estimated as significant.
According to a review of existing literature, the mean prevalence of infantile crying and colic is 17.7% (P25-75: 10.5-21.0%) [18]. Iacono et al. [23] reported an incidence of 20.1% of infants with infantile colic. In this study with the synbiotic formula, the reported prevalence of crying was 15.6% at the age of two months, decreasing to 0.2% at four months of age. A GOS prebiotic-supplemented formula mimicked the effect of human milk in promoting Bifidobacterium and Lactobacillus growth and in inhibiting Clostridium growth, resulting in a significantly lower presence of colic [24]. The use of a partially hydrolysed formula supplemented with FOS and GOS was shown to induce a reduction of crying episodes in infants with colic after 7 and 14 days when compared with a standard formula [25]. We report a low incidence of crying and infantile colic with this new synbiotic formula compared to the reported prevalence in literature.
Interestingly, the administration of a probiotic mixture containing L. acidophilus DDS-1, B. lactis UABLA-12 and FOS was associated with significant clinical improvement in children with atopic dermatitis, with corresponding lymphocyte subset changes in peripheral blood [26]. The evaluation of the incidence and severity of atopic dermatitis with this new symbiotic formula compared to standard infant formula could be a topic for future research.
Since most studies suggest a trend for beneficial clinical effects, and since these ingredients are very safe, prebiotics added to infant formula bring infant formula one step closer to breastmilk, the golden standard [15].









 XML Download
XML Download