

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neonatal jaundice is a common symptom and is usually physiological. However, conjugated hyperbilirubinemia due to obstruction of the extrahepatic bile duct, physically or functionally, requires a prompt diagnostic work-up and management. The most common cause of extrahepatic bile duct obstruction is biliary atresia, accounting for more than 90% of cases [1]. One rare cause is a bile plug, sludge, or stone. Inspissated bile syndrome (IBS) is defined as obstruction of the extrahepatic duct by a bile plug, sludge without bile duct malformation, congenital chemical defects of the bile, or hepatocellular lesions [2]. This inspissation and precipitation of bile and mucus within the bile ducts is usually caused by blood transfusion, prolonged parenteral nutrition, or diuretics [3]. Treatment of IBS generally involves a surgical procedure such as percutaneous transhepatic cholangiography or laparoscopically aided cholecystostomy with irrigation of the common bile duct using normal saline or a mucolytic agent [45]. However, these procedures are invasive, difficult, and frequently accompanied by postoperative complications in infants. Several recent studies have demonstrated that fish oil, which contains omega-3 polyunsaturated fatty acids (PUFAs) affects bile acid metabolism as well as lipid metabolism [67]. For the first time, we herein report that omega-3 PUFAs can be used to treat IBS as an alternative to invasive surgical interventions.
CASE REPORT
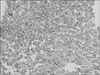
A 5-week-old female infant was admitted for evaluation of jaundice and acholic stool. Her medical history indicated that she was born at a gestational age of 38 weeks with a birth weight of 2,840 g and was admitted to the intensive care unit because of respiratory distress syndrome (RDS) and persistent pulmonary hypertension (PPHN). On day 2, she received a blood transfusion because of anemia. She then underwent ventilator care and received prolonged parenteral nutrition. On day 9, hyperbilirubinemia was present, caused by total bilirubin (TB, 15.9 mg/dL) which decreased to 11.7 mg/dL on day 11 with phototherapy. The levels of direct bilirubin (DB) were normal. However, on day 12, DB level began to increase to 2.1 mg/dL and she was treated with ursodeoxycholic acid (UDCA, 20 mg/kg/day). On day 20, the DB level increased to 5.2 mg, but ultrasound and other laboratory findings were normal. On day 25, RDS and PPHN improved and she was discharged with UDCA. However, jaundice did not improved during follow up. Thus, she was re-admitted for work up. On admission, she weighed 3.05 kg and has been on mixed oral feeding. Her stool was acholic. On physical examination, sclera was icteric. Blood tests revealed the following: hemoglobin, 11.0 g/dL; aspartate aminotransferase (AST)/alanine aminotransferase (ALT), 121/83 IU/L; TB/DB, 6.4/5.5 mg/dL; serum alkaline phosphatase (ALP), 411 IU/L; gamma glutamyltransferase (GGT), 288 IU/L; and bile acids, 120.7 µmol/L. Viral markers (hepatitis A, B, and C viruses; Epstein-Barr virus; toxoplasma; rubella; cytomegalovirus; herpes virus; and human immunodeficiency virus) and syphilis were all negative. Tandem mass neonatal metabolic screening tests (52 items), an anti-nuclear antibody test, and an anti-smooth muscle antibody test were all negative. The findings of an infantogram and abdominal ultrasonography were unremarkable. The administration of UDCA was initiated at 20 mg/kg/day, and the administration of a 20% soybean/medium-chain triglycerides/olive/fish oil emulsion (SMOFlipid®; Fresenius Kabi Austria GmbH, Graz, Austria; 0.6 g α-linolenic acid, 0.6 g eicosapentaenoic acid [EPA], and 0.1 g docosahexaenoic acid [DHA]/200 g fat/L) was initiated at 1 mL/h (1.5 g/kg/d) on the first day of hospitalization. Upon hepatobiliary scintigraphy, biliary excretion into the bowel was somewhat delayed, but bile reached the small intestine within 24 hours (4th hospital day [HD]). Magnetic resonance cholangiopancreatography (MRCP) revealed patent common hepatic and bile ducts (5th HD). On 7th HD, her stool color began to change a little bit yellow color. Follow-up blood tests showed gradual improvement: AST/ALT, 109/69 IU/L; TB/DB, 3.6/3.4 mg/dL; serum ALP, 348 IU/L; and GGT, 266 IU/L (13rd HD). A percutaneous ultrasound-guided liver biopsy revealed bile duct proliferation with bile plugs, hepatocanalicular cholestasis, and a few scattered multinucleated hepatocytes, suggestive of biliary atresia (18th HD) (Fig. 1). This finding forced us to perform intraoperative cholangiography (IOC) despite gradual clinical and biochemical improvement on administration of omega-3 PUFAs for 3 weeks (AST/ALT, 96/60 IU/L; TB/DB, 2.7/2.4 mg/dL). Three weeks after admission, the patient underwent IOC, which revealed a patent gall bladder and common bile duct with passage of bile through the duodenum (Fig. 2). The bile was very thick, and irrigation with normal saline was performed. The stool subsequently became a definite yellow color (21st HD), and blood parameters improved dramatically: AST/ALT, 71/59 IU/L and TB/DB, 1.2/1.0 mg/dL (28th HD). These findings confirmed our final diagnosis. An oral omega-3 PUFA agent, Omacor® (omega-3 acid ethyl ester 90; Kuhnil Pharmacy Co., Cheonan, Korea; 840 mg, comprising EPA-ethyl ester [460 mg] and DHA-ethyl ester [380 mg] per 1-g capsule), was initiated at 500 mg four times per day as a substitute for the SMOFlipid® emulsion. The patient was discharged with Omacor®, UDCA, and multivitamins (30th HD). A follow-up blood test revealed the following: AST/ALT, 47/50 IU/L and TB/DB, 0.3 mg/dL (HD#58). Omacor® was discontinued after 97 days treatment. Throughout the patient's approximately 1-year clinical follow-up with UDCA, the stool color was yellow and the patient remained in good health (AST/ALT, 49/34 IU/L; TB, 0.25 mg/dL) (Fig. 3).
DISCUSSION
Jaundice requiring surgical therapy in young infants may be caused by biliary atresia, choledochal malformation, Caroli disease, and IBS [8]. The diagnosis of IBS is based on the clinical presentation and typical ultrasound findings, which show a dilated extrahepatic bile duct, biliary sludge/plugs, and a distended gall bladder [9]. However, some patients show equivocal or even normal findings [38]. Thus, further investigations such as MRCP and IOC are needed to make a correct diagnosis like this case.
The pathological findings of IBS are nonspecific, but often show evidence of obstruction, such as canalicular bile plugs, bile duct proliferation, and giant cell transformation, as in this case. This finding is considered to be analogous to those seen in other forms of extrahepatic bile duct obstruction (biliary atresia and choledochal cysts). That is, prolonged precipitation of bile within the lumen of the ducts may lead to liver cell cord disruption, hepatocellular necrosis, and giant cell transformation [1].
Although treatment of IBS generally requires surgical intervention, there are therapeutic challenges. In fact, some cases have been reported in which biliary sludge resolved spontaneously without treatment [1011]. However, in this case, we do not believe that the inspissated bile resolved spontaneously. Most cases of spontaneous resolution were dramatically resolved within 1 week, and did not require liver biopsy for diagnosis, whereas in this case, gradual biochemical improvement was achieved over 3 weeks with UDCA and SMOFlipid®, which contained an omega 3-PUFAs. In addition, the pathology findings, which suggested biliary atresia, may have reflected long-term biliary duct obstruction. Some medical trials with UDCA alone to dissolve the bile sludge had failed to improve biochemical tests and ultimately required a surgical procedure [45].
The mechanism of action of omega 3-PUFAs is not fully understood; however, we believe that omega 3-PUFAs may play a role as a choleretic agent and seemed to improve the initial clinical and laboratory findings in this case. Omega 3-PUFAs are well known to effectively prevent and treat parenteral nutrition-associated liver disease. The mechanism includes improved lipid clearance, induction of hepatic fatty acid oxidation, and modulation of inflammation [12]. Several studies have recently reported that fish oil affects not only lipid metabolism, but also bile acid metabolism in humans [613] and rats [714]. In one study, omega 3-PUFAs induced the D-site binding protein and X-receptor alpha, which upregulates cholesterol 7-a hydroxylase, the rate-limiting enzyme in bile acid production and cholesterol excretion [14]. Another study demonstrated that the hepatic induction of bile acid synthesis through Cyp27a1 may upregulate expression of bile acid transporters in both the liver and intestine in rats [7]. Additionally, one study described the effects of fish oil on bile acid metabolism in humans. In a hypertriglyceridemic patient, an increased ratio of the rate of cholic acid synthesis to the rate of chenodeoxycholic acid synthesis increased bile acid synthesis and altered the bile acid distribution in the fish oil-treated group compared with baseline and a bezafibrate therapy group [6].
Given this background, we suggest the possibility of omega-3 PUFAs as a choleretic agent for IBS that can be used as an alternative to surgical intervention. Further investigations are needed on the role of omega 3-PUFAs as a choleretic agent in humans.


 XML Download
XML Download