

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatitis is more commonly encountered in children than ever before, although it remains unclear if the incidence itself has increased or just detection [123]. In contrast to adults, in whom the cause is often idiopathic, pancreatitis in children is usually caused by congenital structural abnormalities, trauma, drugs, and infection [345]. It has been reported that the structural abnormalities of the pancreaticobiliary system, including biliary stones and sludge, are the leading causes of recurrent pediatric pancreatitis [6]. Imaging studies, including ultrasound (US) and computed tomography (CT), are very important for diagnosing pancreatitis and identifying its causes. Generally, CT is superior to US for evaluating pancreatitis, regardless of patient age; however, CT uses ionizing radiation, which does potentially harm growing children. Magnetic resonance imaging (MRI) can be a good alternative for assessing children, and magnetic resonance cholangiopancreatography (MRCP) has become the standard imaging modality for evaluating pediatric patients with pancreatobiliary disease at many institutions. Recent studies have reported that MRCP demonstrates a fairly good correlation with endoscopic retrograde cholangiopancretography or direct cholangiography for delineating several structural abnormalities in the pancreaticobiliary system [78], which encourages the active use of MRCP for assessing in pediatric patients. This article provides a pictorial overview of the MRCP findings of pediatric pancreatitis according to the various causes, with a specific focus on the limitations and possible applications of pediatric MRCP.
MRCP CHARACTERISTICS OF PEDIATRIC PANCREATITIS
Acute pancreatitis
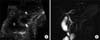
Cross-sectional MRI is useful for assessing the extent of inflammation, peripancreatic fluid collection, and perfusion in the pancreatic parenchyma after administering paramagnetic contrast material. MRCP is indicated to evaluate structural abnormality of the pancreaticobiliary system in pediatric pancreatitis. The normal pancreas demonstrates high signal intensity relative to the liver on T1-weighted fat-suppressed images and low signal intensity relative to the liver parenchyma on T2-weighted images. The signal intensity of the inflamed pancreas is high on T2-weighted images, but remains normal or slightly low on T1weighted fat-suppressed images depending on the severity of pancreatic inflammation. Heavily T2-weighted image is sensitive to demonstrate the signal change of the pancreas parenchyma and peripancreatic fluid collection due to suppression of the fat tissue (Fig. 1A). Diffuse or focal dilatation and a discontinuous pancreatic duct can be seen on MRCP (Fig. 1B), but the small ductal anomalies might be obscured by inflammatory change in the acute stage of pancreatitis. Stones or sludge can be also identified in the pancreatic duct or common bile duct (CBD). In severe cases, there may be parenchymal necrosis and hemorrhage (so- called necrotizing or hemorrhagic pancreatitis) (Fig. 2).
Chronic pancreatitis
Chronic pancreatitis is defined by irreversible architectural and functional changes in the pancreas due to long-standing pancreatic inflammation and injury [6]. It has been noted that chronic pediatric pancreatitis is mainly associated with obstructive and genetic causes [9]. MRCP can identify irregular ductal dilatation with or without stricture, calculi, and pseudocyst (Fig. 3 and 4). However, MRI has some limitations when identifying parenchymal calcifications and small pancreaticoliths or abnormalities in the small distal duct. Therefore, there have been attempts to combine MRI and unenhanced CT in order to diagnose chronic pancreatitis [10].
Pseudocyst
Pseudocyst can present as the complications of pancreatitis in both acute and chronic pancreatitis; they can also present either alone or in multiple. CT is the most sensitive imaging modality for detecting pancreatic pseudocysts, and MRCP is not usually solely used to identify pseudocysts, although it is good at depicting the solid portion within pseudocysts and delineating ductal communication (Fig. 3B).
Hereditary pancreatitis
Hereditary pancreatitis is an autosomal dominant disease that results from mutations in the cationic trypsinogen genes, including PRSS1 and SPINK1 [1112]. Recurrent episodes of acute exacerbation of pancreatitis result in chronic pancreatitis, especially in older children and adolescents. The MRCP findings of hereditary pancreatitis do not differ from those of acute and chronic pancreatitis, depending on the phase of the disease [13]. It is notable that PRSS1 and SPINK1 mutations are associated with pancreas divisum (PD), and these mutations in combination with PD can lead to chronic pancreatitis at an early age (Fig. 3 and 4) [14].
Autoimmune pancreatitis
Autoimmune pancreatitis is histologically characterized by marked fibrosis and the infiltration of CD4-positive T-lymphocytes and immunoglobulin G4-positive plasma cells around the pancreatic duct [15]. Autoimmune pancreatitis is increasingly encountered in adults, but a few cases have been also reported in children and adolescents [16]. The representative characteristics of autoimmune pancreatitis on MR include the diffuse enlargement of the pancreas without focal lesions, multifocal pancreatic duct narrowing, and a peripancreatic hypodense or hypointense rim on contrast-enhanced CT or MRI (Fig. 5A and 5B). Improvement in the radiological findings after steroid therapy may be a diagnostic clue of autoimmune pancreatitis, as it usually indicates a good response to steroids.
Traumatic pancreatitis
Blunt trauma is one of the most common causes of pancreatic injury in children, resulting in >50% of pediatric cases [17]. The body of the pancreas is the most vulnerable site of blunt injury because it can be easily crushed against the vertebral column (Fig. 6A) [1718]. In an acute clinical setting, CT can be modality of choice regarding fast imaging time and accuracy for abdominal traumatic injury. MRI with MRCP is performed when the ductal injury is suspected although CT is the best modality for traumatic pancreatitis in acute clinical setting. Pseudocyst formation is common and has been reported in >50% of patients with traumatic pancreatitis. Approximately 60% of pancreatic pseudocysts are due to blunt trauma [17]. MRI and MRCP can reveal parenchymal changes, including pancreatic fracture, laceration, hemorrhage, pancreatic contusion, peripancreatic fluid collection, hematoma, pseudocyst formation, and other associated injuries in the adjacent abdominal organs (Fig. 6B) [18].
Drug-induced pancreatitis
Drug-induced pancreatitis accounts for up to 12% of cases of acute pediatric pancreatitis [13], but only 0.1-2% of adult cases [19]. Drug-induced pancreatitis is particularly important in children with acute lymphoblastic leukemia (ALL) receiving L-asparaginase therapy, because acute pancreatitis can result. A recent study reported that the high mortality of ALL patients is due to coexisting acute pancreatitis [20]. Cytosine arabinoside treatment, hypercalcemia, and hypertriglyceridemia can also be associated with pancreatitis in ALL patients. Drug-induced pancreatitis also demonstrates a wide spectrum of disease manifestations, from subclinical pancreatitis to fatal hemorrhagic pancreatitis (Fig. 7).
BILIARY CAUSES OF PANCREATITIS
Choledochal cyst
Choledochal cyst (CDC) is a congenital anomaly that manifests as a dilated bile duct. Combination anomalous pancreaticobiliary ductal union (APBDU) and ductal stones can lead to bile reflux into the pancreatic duct which, in turn, predisposes CDC patients to the development of pancreatitis [2122]. MRCP is a valuable tool for preoperative evaluation because it can objectively determine the size, extent, and type of CDC, APBDU, and cholelithiasis, in addition to presence of pancreatitis (Fig. 8 and 9) [723]. The coexistence of CDC and PD is rarely reported (Fig. 10) [24]. On MRCP, CDC appears as a fluid-filled cystic dilation of the bile duct, which is best seen on T2-weighted imaging. CDC is categorized by the Todani classification system as follows [25]: type I (80-90%), cyst confined to the extrahepatic duct (Fig. 8 and 9); type II (3%), diverticulum of the extrahepatic duct; type III (5%), choledochocele, which is the dilatation of the intramural CBD that protrudes into the duodenum (Fig. 11); type IV (10%), multiple cystic dilatations in both the intra- and extrahepatic ducts (Fig. 10); type V, Caroli disease, manifests as multicystic dilatation of the intrahepatic bile duct and may be associated with renal cystic diseases.
Anomalous pancreaticobiliary ductal union
In patients with APBDU, bile reflux can occur due to a dysfunctional sphincter of Oddi or because the common channel becomes obstructed by a stone, sludge, or protein plugs [26]. The maximum length of the normal common channel in children increases with age, and the maximum length of the common channel is reportedly 3 mm in infants and 5 mm in children between 3-15 years of age [2728]. A common channel >5 mm would be considered abnormal in children [7]. It may be difficult to identify APBDU on MRCP, particularly in young patients. A long common channel is represented as a single, tubular, high-signal intensity on MRCP after joining the CBD and pancreatic duct (Fig. 8, 9, 12). However, it may be difficult to identify APBDU on MRCP, particularly in young patients due to small caliber of the bile duct.
Bile duct stone
The majority cases of pediatric pancreatitis caused by bile duct stones are accompanied by structural anomalies in the pancreaticobiliary system, hemoglobinopathy, short bowel syndrome, and total parenteral nutrition [5]. On MRCP, CBD stones can be single or multiple and are typically observed as dark signal-filling defects with or without the dilatation of the bile duct or pancreatic duct. Stones demonstrate various signal intensities on T1-weighted imaging according to their composition (Fig. 8B), while demonstrating dark signal-filling defects on T2-weighted imaging and MRCP (Figs. 8, 9, 10, 12).
Pancreas divisum
Although most patients with PD are asymptomatic, pancreatitis can develop when there is obstruction or stenosis in the accessory ampulla or the dorsal pancreatic duct that drains the major portion of the gland (Fig. 4 and 10) [2129]. In addition, PD can be associated with hereditary pancreatitis and PRSS1 and SPINK1 gene mutations (Fig. 3 and 4) [14]. However, it is questionable about the relationship between the high incidence of pancreatitis and the presence of PD [293031]. In patients with complete PD, the dorsal and ventral ducts are completely separated (Fig. 4), whereas incomplete divisum maintains a connection via the small branches (Fig. 12).
PITFALLS OF PERFORMING PEDIATRIC MRCP
Respiratory motion artifacts
Respiratory motion artifacts are the most frequent cause of inadequate MRCP imaging, resulting in blurring and ghosting (Fig. 13) [283233]. This motion can result in inconsistent image quality because certain structures cannot be properly found in each sampled k-space, which can cause misdiagnosis because the normal pancreatic duct appears disconnected, stenotic, or dilated [34]. Respiratory motion artifacts can be minimized using the respiratory triggering technique. However, respiratory triggering lengthens the total scan time, especially in patients with irregular respiration due to respiratory misregistration. Moreover, averaging up to six excitations can reduce motion artifacts, although this also increases the scanning time.
Low signal-to-noise ratio
Long echo time and echo train, small-caliber pancreaticobiliary duct, and respiratory motion artifacts contribute to low signal-to-noise ratio (SNR) on pediatric MRCP. Images with low SNR are dark and grainy, resulting in poor visualization of the pancreaticobiliary duct (Fig. 13). The general principles used to improve SNR on MRCP include averaging additional signals and using the proper field of view, greater number of phase-encoding steps, a highfield MR scanner, 3-dimensional (3D) MR sequencing, and selecting an appropriately sized radiofrequency coil [35].
Small-caliber pancreaticobiliary duct
Neonates and young infants have small bile ducts that measure approximately ≤1 mm in diameter, and the pancreatic duct is even smaller than the bile duct in normal patients. Such small structures produce fewer signals and tend to be more susceptible to respiratory motion artifacts. These problems could be solved using strategies that improve the SNR and reduce motion artifacts. In addition, secretin-stimulated MRCP can improve visualization of the pancreatic duct by triggering transient dilatation (Fig. 14) [10323637].
Overlapping with nearby fluid-filled organs
Fluid in the stomach, duodenum, small and large intestines, kidneys, and the cerebrospinal fluid in the spinal canal can be identified on MRCP (Fig. 12B and 15A). Pathological conditions such as a large number of ascites, periportal and peripancreatic fluid collections, and distended gallbladder also affect the visibility of the pancreatic duct. Such fluid can be reduced by fasting, choosing adequate slab thickness depending on the patient's body habitus (Fig. 15B), 3D sequencing with postprocessing (Fig. 15C), and administering negative oral contrast media such as ferumoxil oral suspension, ferric ammonium citrate, or pineapple juice [1032353839].
CONCLUSION
Various structural abnormalities of the pancreaticobiliary system contribute to the development of pancreatitis in children and they can be effectively evaluated by MRI and MRCP. In addition, MRI including MRCP is attractive imaging modality for use in children as it is free of radiation exposure and iodine contrast agent. Therefore, pediatric physicians and pediatric radiologist should be familiar with using MRCP to evaluate pancreatitis and its etiology in children.














 XML Download
XML Download