

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chest pain in the pediatric population is not rare and is mostly a benign symptom. The causes of chest pain are diverse, and formulating a differential diagnosis is not easy. In most cases pediatric chest pain is either idiopathic or is caused by benign diseases. This is not the case for adults, in whom chest pain is usually the result of more aggressive diseases [123]. But, few clinical studies have addressed the causes and clinical characteristics of pediatric chest pain. The most common causes are musculoskeletal diseases, pulmonary diseases, and idiopathic cases. Less common cause are gastrointestinal diseases and cardiac diseases [4]. The situation in Korea is similar [5].
Sabri et al. [6] suggested that there is a higher proportion of upper gastrointestinal (UGI) disease among children and teenagers with chest pain, and recommended including a clinical examination focusing on GI disease to determine the true source of chest pain.
The aim of this study is to evaluate the causes of chest pain in children and to determine the usefulness of several diagnostic examinations used in formulating the differential diagnosis of pediatric chest pain.
MATERIALS AND METHODS
We retrospectively surveyed 75 children (42 males, 56.0%; 33 females, 44.0%) mainly presenting with chest pain who visited the pediatric clinic of Hanyang University Hospital (Seoul, Korea) from January 1995 to March, 2015 Children 9-14 years of age (57.3%) were most common, followed by 6-year-olds (14.7%) (Fig. 1).
Data on clinical history, physical examination, chest X-ray, and electrocardiography (ECG) were reviewed for each patient using outpatient records. Thorough cardiovascular examinations (including 24-hour Holter monitor recording, echocardiography, and exercise stress test), and UGI examinations (endoscopy, gastroesophageal scan, 24-hour esophageal pH monitoring) were performed in select patients depending on specific history and clinical status.
We investigated what diseases and organ diseases were the primary causes of chest pain in these children, and how valuable the diagnostic procedures were in terms of differential diagnoses. A simple abnormality in a clinical examination without true correlation was not regarded as the primary cause of the symptom. We made the final diagnoses in the patients according to the symptomatic improvement in 6 months upon specific treatment and whether the symptoms recurred or not afterwards. This study was approved from the institutional review board of Hanyang University Hospital (IRB No. HYUH 2015-07-029-001).
Statistical analysis
General descriptive statistics of patients are presented as frequencies and percentages (%). The prevalence and the proportion were evaluated by the exact or normal approximation test to test the hypothesis of a single population proportion, and the comparison of means was conducted using the Wilcoxon rank-sum test. All the tests are bilateral at a significance level of α=0.05. All statistical analyses were performed using SAS ver. 9.3 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Gastrointestinal endoscopy was performed in 57 patients. Of these, 48 patients showed obvious mucosal lesions. These patients subsequently underwent further GI examinations, gastroesophageal scan, and 24-hour esophageal pH monitoring. The mucosal lesion sites of these patients were mainly esophageal: reflux esophagitis (n=27), acute erosive esophagitis (n=8), esophageal ulcer (n=7), nodular gastritis (n=3), and gastric ulcer (n=3). Eight (16.7%) among these 48 patients also showed positive Helicobacter pylori infections. Accompanied endoscopic findings in addition with the above were chronic superficial gastritis in 13 cases, duodenogastric reflux in 12, chronic duodenitis in 10, and duodenal ulcer in one.
The prevalence rate of H. pylori in these children showed statistical significance (p<0.001) compared with the rate in children with chronic abdominal pain (6.7%, 2011-2014) and in the general population of children (5.8%, 2011-2014) (Table 1) [7].
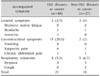
The most common cause of the chest pain was esophago-gastric diseases (64.0%; esophageal 56.0%, gastric 8.0%), followed by idiopathic cases (16.0%), cardiac diseases (12.0%), chest trauma (4.0%), respiratory diseases (2.7%), and psychiatric disease (1.3%). Among the children presenting with chest pain, the proportion finally diagnosed as esophago-gastric diseases was significantly higher than half (p=0.015). The mean age of the children with esophago-gastric diseases was higher than that of the children with other diseases, but not statistically significant (p=0.056) (Table 2).
ECG was performed in all patients, of whom 21 (28.0%) showed abnormalities. Sinus arrhythmia was most commonly noted, right bundle branch block (RBBB) in three, with one patients each displaying ST elevation, left axis deviation, PR prolongation, left ventricular hypertrophy, and right axis deviation. Only two cases of sinus arrhythmia showed the same abnormality in 24-hour Holter monitoring; one case with RBBB and one case with PR prolongation were in ventricular septal defect (VSD) status with normal findings in echocardiography. Echocardiography performed in 34 children revealed nine abnormalities including three VSD, one aortic regurgitation, one atrial septal defect, one septal hypertrophy, and one high overload. Twenty four-hour Holter monitoring was performed in four, of whom two showed sinus arrhythmia (Table 3).
Chest X-ray performed in all patients revealed abnormalities in three, consisting of one each of enlargement of pulmonary conus, bronchopneumonia, and cardiomegaly due to VSD. The patient with enlargement of pulmonary conus was diagnosed as pulmonary tuberculosis and in the echocardiography. Aortic regurgitation was also noted, and prompted a clinic with complaint of chest pain 5 years later (Table 4).
The patients whose primary diseases were esophageal or gastric had accompanying symptoms that most often were nausea (n=8) and vomiting (n=6). Patients whose primary diseases were not UGI diseases showed few GI symptoms. There was no distinct difference concerning general symptoms and thoracic symptoms between children with and without primary UGI diseases (Table 5).
After the final diagnoses of chest pain, patients were followed-up for at least 6 months to assess whether symptoms disappeared with treatment, persisted, or recurred after initial improvement. Chest pain was improved with GI medicines in 37 patients (49.3%). Of these 37, 13 (35.1%) showed abnormalities in their cardiac examinations, which eventually showed little clinical correlation as a cause of chest pain. We continued to observe 24 patients (32.0%) who were not treated and did not display symptom recurrence; eight showed abnormal findings in their cardiac examination but did not require specific treatment. Three improved but the symptoms recurred, three (4.0%) suffered from sustained chest pain despite GI medicine, in whom abnormal cardiac examination results were already reported and might be the main reason for the persistence of symptoms. In three patients chest pain spontaneously resolved without any treatment (Table 6).
DISCUSSION
Chest pain in children is not a frequent symptom, as in adults. Pediatric chest pain usually present around 10-years-of-age [18910], and females present more commonly than males. In this study, the majority of patients were 9 to 14-years-of-age (57.3%) and 6-years-of-age (14.7%). The male and female ratio was about 4:3.
Children with chest pain are usually referred to pediatric cardiologists, but chest pain is not an important or frequent symptom in children with cardiac diseases [41112]. Careful history-taking, physical examination, and diverse laboratory investigations are required to determine the etiology of chest pain [131415]. Musculoskeletal diseases (trauma, severe muscle sprain), respiratory diseases (pneumonia, pleuritis, asthma, chronic cough), UGI diseases (esophagitis, gastrointestinal reflux disease, foreign body, esophageal spasm, peptic ulcer disease), cardiovascular diseases (cardiomyopathy, endocarditis, valvular diseases, myocardial ischemia), and idiopathic causes are included in the differential diagnosis [4]. Idiopathic chest pain is most common in girls around 10-years-of-age [16].
Rowe et al. [17] studied clinical characteristics and causes of chest pain in 325 children visiting the emergency room. The most common cause was idiopathic (33%), followed by chest wall pain (28%), respiratory disease (19%), trauma (15%), and psychogenic (5%). Very few patients (2%) were hospitalized and there were no patients with cardiovascular disease. There have been several studies regarding the causes of pediatric chest pain; in most of these UGI endoscopic examinations were seldom done so detailed explanations concerning the primary problems are lacking.
Chest pain caused by cardiovascular disease is not common in children with an incidence of 4% to 6% [18]. Mitral regurgitation is a major cardiac cause of chest pain in children, and is accompanied by vertigo, dyspnea, anxiety, and palpitations [19]. In this study, diverse examinations were performed to investigate cardiovascular disease, but clinically pathologic cardiac disease was not a major cause.
Several recent studies have suggested that UGI disease should be included in the differential diagnosis of chest pain [620212223]. Hsia et al. [21] performed UGI endoscopy and esophageal manometry in 100 patients with non-cardiac chest pain and diagnosed 24 cases of esophagitis, 18 cases of gastritis or duodenitis, 14 cases of esophageal hernia, and six cases of peptic ulcer disease, and recommended specific examinations for UGI disease in non-cardiac chest pain. Berezin et al. [22] diagnosed UGI diseases in 78% of 27 patients whose causes were specific; these patients showed clinical improvement after the treatment of the UGI diseases. In this study, UGI disease was suspected in 18 children, and evaluations specific for the UGI diseases were performed. Specific UGI diseases were diagnosed in all these children and the symptoms improved after proper treatment. Lipsitz et al. [24] reported that psychosomatic anxiety disorders could be major causes of non-cardiac chest pain in children; however, further evaluation for UGI disease was not done. The authors reported the diagnostic efficacies of several examinations for pediatric chest pains in 2003 [25]. In the former study, the evaluation of UGI diseases were performed only in 18% of patients of the overall patient study group, and idiopathic cases were most common. Performing more examinations to determine whether UGI disease is a cause of cardiac pain, as UGI diseases were shown to be major causes of chest pain in children in this study. That is, the idiopathic causes of chest pain were less than 20%, while UGI disease caused chest pain in 40% of all cases in this study.
In our study, the incidence of H. pylori among the children with UGI diseases was higher than that among those with chronic abdominal pain in Korean children. We could not find our similar study performed in Korean children, but it was already reported that H. pylori infection have a important role in non-cardiac chest pain from Asia-Pacific survey [26].
Study limitations include the retrospectively design, lack of complete laboratory examinations in some patients, and failure of a specific treatment for certain organ disease to alleviate patient suffering. More differential diagnostic plans are needed, and should be investigated using a well-designed protocol.
In conclusion, careful history taking, physical examination, and proper clinical interventions are usually required to determine the diverse causes of chest pain. GI evaluation, including UGI endoscopic examination, is recommended to diagnose esophageal and gastric diseases in patients with non-cardiac chest pain.






 XML Download
XML Download