

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A fecaloma is a laminated mass of accumulated feces that is much harder in consistency than a fecal impaction [1]. Fecalomas are usually located in the sigmoid colon or rectum, but rarely in the cecum [23]. Most fecalomas are successfully treated by conservative procedures such as laxatives, enemas, and rectal evacuation [2]. However, when conservative treatments fail, surgical intervention may be needed [4]. We report an ileal fecaloma in a 10-year-old male; the fecaloma induced small bowel obstruction and required surgical intervention. To our knowledge, this is the first report of such a case in the English literature.
CASE REPORT
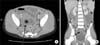
A 10-year-old male was admitted because of rapidly developing abdominal pain which, with fever, vomiting and diarrhea, had commenced 1 week prior. He had a history of chronic constipation with about 2 bowel movements per week and hard stool for few years. And medication for constipation was done randomly. He appeared pale; however, his vital signs were stable. His abdomen was distended and bowel sounds were increased. Tenderness was evident over the whole abdomen, but none of rebound tenderness, guarding, or rigidity was evident. Blood test data were as follows: hemoglobin, 7.1 g/dL; hematocrit, 28%; mean corpuscular volume, 54.4 fL; serum iron, 13 µg/dL; total iron-binding capacity, 394 µg/dL; ferritin, 3.21 ng/mL; white blood cell count, 7,680 cells/mm3 (neutrophils, 71%); blood urea nitrogen, 15.3 mg/dL; creatinine, 0.8 mg/dL; sodium, 132 mmoL/L; potassium, 4.1 mmoL/L; chloride, 98 mmoL/L; total CO2, 15 mmoL/L; and C-reactive protein, 0.05 mg/dL. Other data were not remarkable. A simple abdominal x-ray revealed multifocal air-fluid at the mid-abdominal level, and distended small bowel loops (Fig. 1). An abdominal pelvic computed tomography (CT) scan taken on the second hospital day revealed mechanical small bowel obstruction at the distal ileum, with a transition zone (Fig. 2). In this obstructed area, we delineated hypodense mass structure; however, we couldn't identify what it was. The abdominal pain was not relieved, and bilious vomiting continued, upon application of nasogastric tube drainage. An abdominal x-ray performed on the third hospital day showed that the mechanical ileus had become increasingly aggravated.
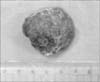
Emergency surgery was performed on the same day, and a 4×3×2.5 cm fecaloma (Fig. 3) was found in the lumen of the distal ileum 65 cm proximal to the ileocecal valve and any other anatomical lesions (e.g., ileal atresia, ileal stenosis) were not found in operative finding. The small intestine proximal to the fecaloma obstruction was markedly distended. After the removal of the fecaloma via enterotomy, all symptoms of mechanical intestinal obstruction resolved completely. After discharge, he was treated for constipation over 6 months without complications, including fecaloma.
DISCUSSION
Although fecal impaction is common and disturbing, fecaloma is an extremely rare form of impaction, referring to an accumulation of fecal material that forms a mass separate from other bowel contents [1]. Fecalomas have been described in patients suffering from chronic constipation, Hirschsprung's disease, Chagas' disease, inflammatory diseases, neoplastic diseases, and psychiatric diseases [5]. Our present patient complained of chronic constipation, but the underlying cause was unclear.
Fecalomas occur most commonly in the rectosigmoid area; the small bowel is a most unusual site [2]. This may be explained by the fact that stools in the left colon are firmer than those in other regions, because the colon diameter is narrower on the left than the right [46]. In our present case, the fecaloma developed in the distal small intestine, provoking rapidly progressing mechanical obstruction of small intestine. However, we couldn't find any underlying small intestinal lesion related to fecaloma. To our knowledge, this report is the first in the English literature to describe an ileal fecaloma inducing mechanical small bowel obstruction, requiring surgical intervention.
The symptoms of fecaloma are usually nonspecific, including the "overflow" type of diarrhea, constipation, weight loss, and vague abdominal discomfort after meals [7]. Fecaloma diagnosis is usually made radiologically when the characteristic intraluminal mass is noted on plain x-rays, barium enema, or abdominal CT [2]. Such masses have smooth margins and are not attached to the mucosal surface, thus moving within the bowel lumen [8]. Serious complications may result; these include colonic obstruction, perforation, sciatica, ureter obstruction, secondary hydronephrosis, and deep vein thrombosis [9]. Commonly, fecalomas can be treated using conservative methods such as laxatives, enemas, and digital evacuation. However, surgical intervention may be required for fecaloma removal in some intractable cases like this patient [9].
A fecaloma in the small intestine is extremely rare. However, this should be considered in differential diagnosis when symptoms of acute mechanical small intestinal obstruction develop in a child with constipation.

 XML Download
XML Download