

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gilbert syndrome (GS) is a common hereditary disorder of bilirubin metabolism due to reduction of uridine diphosphate-glucuronyl transferase 1A1 (UGT1A1) activity, often to 30% of the normal level. It is characterized by unconjugated hyperbilirubinemia in the absence of liver disease or hemolysis [1,2]. Hereditary spherocytosis (HS) is the most common inherited hemolytic anemia due to red cell membrane defect leading to premature cell destruction. About 75% of HS patients have autosomal dominant inheritance. The patients have variable degrees of anemia, jaundice, and splenomegaly. The severity varies from asymptomatic to severe hemolytic anemia [3]. The co-inheritance of GS with other clinical conditions such as spherocytosis, thalassemia, or cystic fibrosis is associated with higher levels of bilirubin and increased tendency to form gallstones [4]. Here, we report a case of coexistence of GS with HS in a child who presented with extreme jaundice.
CASE REPORT
A 12-year-old boy was referred to Chosun University Hospital for nausea and jaundice that began 3 days before admission. He had no history of anemia or jaundice and none of his family members had anemia or jaundice.
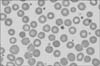
His physical examination showed extreme jaundice and hepatosplenomegaly. His laboratory findings were as follows: hemoglobin (Hb), 13.3 g/dL; hematocrit, 35.4%; white blood cells, 9,940/mm3; platelet, 302,000/mm3; mean corpuscular volume, 78.4 fL; mean corpuscular Hb concentration 37.5 g/dL, and reticulocyte count 15.7%. Peripheral blood smear showed small and dense spherocytes (Fig. 1). The results of liver function tests revealed that the serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, gamma glutamyl transpeptidase, and total/direct bilirubin were 146 IU/L, 458 IU/L, 357 U/L, 175 U/L, and 42/16 mg/dL, respectively. The lactate dehydrogenase level was 851 IU/L and haptoglobin level was below 28 mg/dL. The results of other tests, including levels of vitamin B12, folic acid, serum iron, and ferritin; total iron binding capacity; Coombs direct and indirect tests; and Hb electrophoresis were also normal. Incubated osmotic fragility was increased (beginning, 0.8%; ending, 0.55%). Abdominal ultrasonography showed hepatomegaly (151 mm), splenomegaly (170 mm), and multiple gallstones. Based on the presence of spherocytes and increased osmotic fragility and the absence of any other cause of the hemolytic anemia, the diagnosis of HS was made.
On the 28th day after admission, the patient's jaundice gradually improved. The serum levels of AST, ALT, and total/direct bilirubin were 42 IU/L, 54 IU/L, and 9/1.2 mg/dL, respectively. Because the child had extreme jaundice and multiple gallstones in the absence of severe anemia, we further examined another cause of unconjugated hyperbilirubinemia. Laboratory investigations for immunoglobuin M (IgM) antibody to hepatitis A virus, hepatitis B surface antigen, anti-hepatitis C virus antibody, IgM antibody to Epstein-Barr virus viral capsid antigen, anti-cytomegalovirus IgM, and anti-herpes IgM were all negative. The serum levels of copper and ceruloplasmin were 110 µg/mL (normal, 70-130 µg/mL) and 26.1 mg/dL (normal 20-60 mg/dL), respectively. The mutation of ATP7B gene was not detected. The possibility of GS was considered. DNA analysis revealed the (TA)7/(TA)7 genotype as seen in patients with GS, thus confirming the diagnosis of GS. Therefore, the child was diagnosed with coexistence of HS and GS. He underwent laparoscopic cholecystectomy and splenectomy. He did well postoperatively and did not experience any complications at the 36-month follow-up.
DISCUSSION
GS is common hereditary disorder of bilirubin metabolism. Its estimated prevalence is approximately 3% to 7% in the general population [5,6]. GS is more common in males than in females, possibly owing to a relatively higher level of daily bilirubin production in males. It is often diagnosed after puberty when the endogenous steroid hormones affect bilirubin metabolism, leading to an increase in the serum level of bilirubin [7]. GS is the result of a mutation in the gene for the enzyme UGT1A1. The mutations of UGT1A1 decrease the activity of the UGT1A1 or decrease the amount of the UGT1A1 in the liver, leading to unconjugated hyperbilirubinemia. An elongated TA repeated A[TA]7TAA (UGT1A1*28) is the most common genetic cause of GS in Caucasians [8]. Maruo et al. [9] reported linkage of GS to A[TA]7TAA (UGT1A1*28) and T-3279G (UGT1A1*60). The missense mutations 211G>A has been reported to be associated with GS in the Asian population. [10]. In Korea, genetic mutations of GS have been reported in 5 cases including our case; 2 cases had homozygous for A[TA]7/7TAA (our case), 2 cases had compound heterozygosity (T-3279G and G211A), and 1 case had three heterozygosity (T-3279G, A[TA]7TAA, and G211A) [11,12,13,14].
GS is characterized by a fluctuating increase in indirect bilirubin levels during fasting, stress, dehydration, menstruation, and overexertion. Other than experiencing jaundice, patients are typically asymptomatic. The serum levels of total bilirubin are most often <3 mg/dL, although in the setting of increased bilirubin production, the levels may be higher but usually <6 mg/dL [2].
HS is the most common inherited hemolytic disorder characterized by the loss of membrane surface area, leading to reduced deformability due to defects in the membrane proteins ankyrin, band 3, spectrin, and protein 4.2 [15]. Spherocytes are vulnerable to splenic sequestration and destruction. The common clinical findings are anemia, jaundice, and splenomegaly. Although the degree of anemia is variable and may be absent, mild, moderate, or severe, most patients present with well-compensated hemolytic anemia [3]. Common complications are cholelithiasis, hemolytic episodes, and aplastic crises. Splenectomy is the treatment of choice for moderate to severe forms of the disease. Splenectomy results in increased Hb level, decreased need for transfusion, decreased reticulocytosis, and fall in the serum level of bilirubin and likelihood of gallstone formation although red cell survival remains shortened [15,16].
According to the guidelines of HS [3], patients with mild HS have no anemia, mild reticulocytosis, and little jaundice (Hb level from 11 to 15 g/dL, reticulocyte count from 3% to 6%, and total bilirubin level from 1 to 2 mg/dL). In contrast, patients with severe HS have marked reticulocytosis, anemia, and hyperbilirubinemia (Hb level from 6 to 8 g/dL, reticulocyte count more than 10%, and total bilirubin more than 3 mg/dL). Although our patient had mild HS with normal Hb, he had an extremely high serum level of bilirubin. This discrepancy suggested that other conditions were associated with unconjugated hyperbilirubinemia, especially inherited deficiency of hepatic glucuronosyltransferase. In such cases, further evaluation should be performed. In light of the individual prevalence rates (GS, 3-7%; HS, 1/2,000 persons), the calculated rate of coexistence of 2 diseases is almost 15-35 per million births [17]. In Korea, only two adult cases have been reported in the literature and this is the first case report in the children [12,14]. Patients with simultaneous presence of HS and GS have bilirubin levels higher than those with either abnormality (total bilirubin level from 10 to 15 mg/dL) [12,18,19]. In our patient, the serum level of total bilirubin was higher than previous report. It was probably due to cholelithiasis. Del Giudice et al. [20] reported that patients with HS, who coinherited GS, had almost 5-fold greater tendency to form gallstones than normal HS patients. Our patient also had multiple gallstones. Splenectomy is performed in cases of severe HS and considered in cases of moderate HS. The gall bladder should be removed concomitantly if there are symptomatic gallstones [3]. Combined splenectomy and cholecystectomy should be considered in case of coexistence of GS and HS.
In conclusion, we presented a case of coexistence of GS and HS in a 12-year-old boy. The possibility of the coexistence of GS and HS should be considered in patients with inappropriately high serum bilirubin levels when compared with the severity of HS.
 XML Download
XML Download