

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epiploic appendagitis is a benign clinical rarity with 8.8 incidences per million people [1]. Epiploic appendages are fat-filled, serosa-covered structures positioned in two separate longitudinal lines along the colon; inflammation can be caused by torsion or thrombosis in the appendageal draining vein [2,3,4,5,6]. Abrupt onset of abdominal pain over the corresponding area is a major symptom of epiploic appendagitis [5]. Epiploic appendagitis has been reported in children and adolescents; however, it is not accompanied by other gastrointestinal diseases [7]. This report describes a case of epiploic appendagitis accompanied by acute gastroenteritis in an eight-year-old girl.
CASE REPORT
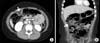
An eight-year-old girl who had been healthy with a body mass index of 29 kg/m2 was admitted to the hospital due to abdominal pain in the right upper quadrant for one day, which was progressively increasing in intensity. She had intermittent fever, with 8 to 10 episodes of non-bilous, non-projectile vomiting and frequent watery diarrhea with urgency over the last two days. On admission, she had a fever (38.6℃), pulse rate of 70 beats/min, and respiration of 20 breaths/min. Physical examination revealed tenderness and rebound tenderness in the right upper quadrant. Decreased bowel sounds were heard on auscultation. Laboratory studies were unremarkable, except for leukocytosis with a predominance of neutrophil, 14,100/mm3 (neutrophil 79.5%, lymphocyte 12.2%, and monocyte 6.5%) and an elevated C-reactive protein level, 4.32 mg/dL (reference range, 0-0.3 mg/dL). Blood and leukocytes were not found in stool and stool culture was sterile. Although no organism was isolated from stool examination, based on symptoms, we diagnosed the patient as acute gastroenteritis, and intravenous hydration, empirical antibiotics (intravenous amoxicillin/clavulanate), and antidiarrheal agents were administered. Due to right upper quadrant tenderness, abdominal contrast computed tomography (CT) scan was performed, which demonstrated a 2.2-cm ovoid fatty mass surrounded by an enhanced line with minimal haziness observed in the adjacent tissue (Fig. 1) in the ascending colon, and epiploic appendagitis was diagnosed. The patient was managed conservatively with hydration, antibiotic therapy, and antidiarrheal agents. On the third day after admission, fever, vomiting and abdominal pain were resolved and stool frequency decreased. On the fifth day, the patient was discharged from the hospital without complications.
DISCUSSION
Epiploic appendages are pendant structures protruding from the serosal layer of the large intestines, supplied by end arteries of long vessels of the colon and the tortuous vein drains. Excessive movements affecting the epiploic appendages may limit the blood supply and lead to torsion. As a result of spontaneous thrombosis in the vein, epiploic appendages can become infarcted as well. Torsion of the epiploic appendage or thrombosis in the draining vein of the epiploic appendage can cause epiploic appendagitis [2,3,4,5,6].
Epiploic appendagitis can affect any age group, with a peak incidence in the fourth to fifth decade, and obesity and heavy exercise are contributing factors [3,8,9]. The typical clinical manifestation of epiploic appendagitis is abdominal pain that is acute, moderate to severe, colicky, and continuous over the corresponding area of the colon. Sometimes there is vomiting; however, fever and diarrhea are unusual. Localized tenderness over the site is common and often associated with rebound tenderness without rigidity [2,5,6]. These symptoms mimic appendicitis, cholecystitis, and diverticulitis [2,3,10,11,12].
In the current case, an eight-year-old girl with a body mass index of 29 kg/m2 whose symptoms included fever, vomiting, diarrhea, and abdominal pain was found to have epiploic appendagitis. How obesity contributes to the development of epiploic appendagitis is unclear, but persons with visceral fat are more inclined to have a limited blood supply or venous thrombosis in their outpouching structure along the large intestine. Based on the symptoms, the patient was diagnosed with acute gastroenteritis. An abdominal CT was performed to differentiate her condition from appendicitis or right-sided diverticulitis. On the CT, ovoid fatty mass was observed in the ascending colon, corresponding to the tender point. We can conclude that epiploic appendagitis was the cause of acute abdominal pain. Although secondary epiploic appendagitis may occur as a result of appendicitis, cholecystitis, diverticulitis, or pancreatitis, most cases are not associated with other gastrointestinal diseases. Considering that fever and diarrhea are not uncommon in epiploic appendagitis, in the current case, epiploic appendagitis was not encountered secondary to acute gastroenteritis, but was incidentally accompanied by acute gastroenteritis.
Laboratory investigations are not conclusive. Radiologic evaluations, abdominal ultrasound examinations, and CT are useful in diagnosis. The presence of a hyperechoic non-compressible ovoid structure near the colonic wall with the absence of blood flow in a sonographic assessment provides a clue for diagnosis. An ovoid fatty mass with a hyperattenuated ring sign is a distinctive CT finding, which may enable clinicians to differentiate epiploic appendagitis from diverculitis and other diseases causing acute abdominal pain [10,11,12]. Adjacent to the lesion, fat stranding, a mass involving the bowel wall, and thickening of the peritoneum are frequently observed [13]. Epiploic appendagitis resolves spontaneously within five to seven days without surgery; however, if the diagnosis is made during exploration, the best strategy is to remove the affected area [14]. The patient in this report was diagnosed with epiploic appendagitis by contrast CT and was treated successfully with conservative management.
Predominantly, epiploic appendagitis is a self-limiting disorder, and it is important that pediatricians and radiologists become familiar with it to prevent not only the overuse of medicinal resources, but also unnecessary hospitalization and surgical intervention.
 XML Download
XML Download