

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urinary tract infection (UTI) is an infection that affects part of the urinary tract. Pyelonephritis can lead to pyonephrosis, urosepsis, renal failure and death. In complicated cases, urosepsis occurs in 10% of children with UTI.
The liver plays important role in the defense against systemic infections; 2 mechanisms are involved in this action. First, Kupffer cells in the liver play a key role in the hepatic detoxification of bacterial endotoxin or lipopolysaccharide [1-3]. Second, the liver removes bacteria from the circulation [2]. That process occurs mainly through the reticulo-endothelial system of the liver [4]. Because of the liver's defense mechanism, it is important to maintain liver function during infections such as UTI.
Liver dysfunction is common in patients with sepsis and ranges from mild elevations of serum aminotransferases to severe cholestasis. There is a classic description of neonatal cholestasis in the context of an UTI in the literature, but this description limited to jaundiced patients alone and not related to liver dysfunction [5].
The aim of this study was to evaluate the prevalence of increased aminotransferase levels and investigate the association of increased aminotransferase levels with the type of antibiotics, degree of vesicoureteral reflux (VUR), and causative organisms in children admitted to hospital with an UTI.
MATERIALS AND METHODS
Study design
The study included patients with a diagnosis of UTI who were admitted to the Konyang University Hospital from January 2007 to May 2011.
UTI was defined as a positive urine culture (>105/colony forming unit [CFU]) of a single strain and associated symptoms, especially, pyrexia (body temperature≥38℃). Sterile urine was obtained through a sterile urine collection bag, and serum samples were obtained within the first 24 hours after admission. Patients with neonatal jaundice and other liver disease were excluded.
Routine treatment included the administration of intravenous antibiotics such as ampicillin/sulbactam, aminoglycoside, cephalosporins (cefotaxime or ceftriaxone) or vancomycin. The normal reference ranges of serum aspartate-aminotransferase (AST), alanine-aminotransferase (ALT) and total bilirubin were ≤50 IU/L, ≤50 IU/L and <1 mg/dL, respectively. Acute pyelonephritis (APN) was diagnosed by kidney sonography, abdomen computed tomography or dimercaptocuccinic acid scan.
We collected patients and obtained data through chart review retrospectively. There were 249 patients diagnosed with UTI, among them, aminotransferase levels were increased in 51 patients at the time of admission. And we investigated the association of increased aminotransferase levels with the type of antibiotics, degree of VUR, and causative organisms.
Statistical analyses
Statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Comparisons between groups were performed using the Independent-samples t-test, chi-square test, and Fisher's exact test. Data were expressed as mean±standard deviation for continuous variables. Statistical significance was set at p<0.05.
RESULTS
Demographic and clinical characteristics of patients
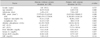
The mean age of patients was 15.88±28.21 months, and the mean duration of hospitalization was 6.73±2.36 days. There were 149 boys (59.8%) and 100 girls (40.2%). The maximum values of aminotransferase were 559 IU/L for AST and 538 IU/L for ALT. Escherichia coli was the most common causative organism of UTI (Table 1).
Factors associated with increased aminotransferase levels
A comparison of multiple factors between patients with and without increased aminotransferase levels is shown in Table 2. Patients with increased aminotransferase levels were younger than those with normal levels (chi-square test, p=0.00). Segmented neutrophil count and serum creatinine level were higher in patients without liver enzyme elevation (p=0.001, p=0.027, respectively). But, lymphocyte count was lower in these patients (p=0.001). However, unlike age, other factors such as segmented neutrophil count, lymphocyte count, and serum creatinine level had relatively small differences. Also, this difference was present in the normal range. Therefore, the age of patients was only meaningful factor that showed difference between 2 groups. There were no significant differences in the causative organism, regimen of antibiotics, degree of VUR and occurrence of APN between 2 groups (Tables 3-5).
Long-term follow-up of aminotransferase levels
In most children, abnormal aminotransferase levels normalized during convalescence without the need for any further management. There were 16 cases of failed follow-up. Apart from these, only 2 patients still had increased aminotransferase levels when they left hospital. The aminotransferase levels became normal ranges at 6 weeks in 1 patient and at 2 months in another patient (Fig. 1). The Fig. 1 presented the aminotransferase levels for total observation period.
DISCUSSION
The liver is a large, complex organ that plays a central role in the metabolism of carbohydrates, proteins and fats and in detoxifying the waste products of metabolism. In addition, the liver is responsible for synthesizing and secreting bile, synthesizing lipoproteins and plasma proteins, and maintaining a stable blood glucose level [6,7].
The mechanism underlying the development of hepatic dysfunction can be divided into 2 phases. In patient with sepsis, the primary phase of hepatic dysfunction occurs in the initial state. In this stage, decreased cardiac output and mesenteric arterial vasoconstriction reduce both portal and systemic circulation. Consequently, hepatic hypoperfusion occurs, and this leads to dysfunction of the liver [8,9]. Because of enzyme leakage from acute cellular and mitochondrial injury, elevated aminotransferase levels are common in patient with primary hepatic dysfunction; however, this injury is mainly caused by hemodynamic problems, and can be successfully treated with proper resuscitation [9]. The secondary phase of hepatic dysfunction occurs with the interaction between Kupffer cells, hepatocytes, neutrophils, and endothelial cells as a response to systemic infection. These cells are activated by local inflammation and produce proinflammatory cytokines, eicosanoid mediators, reactive oxygen products and nitric oxide. Furthermore, these products aggravate the inflammatory response and increase coagulation activities [2,10].
Several studies have reported the association between systemic infection and cholestasis in infants and children. Related organisms include aerobic and anaerobic gram-negative and gram-positive bacteria such as Escherichia coli, Klebsiella pneumonia and Pseudomonas aeruginosa, with gram-negative bacteria causing most of the infections [11]. In the present study, Escherichia coli was the most common causative organism (76.7%). The primary site of infection is intra-abdominal in most cases, but other sites of infection such as UTI, pneumonia, endocarditis and meningitis have been associated with jaundice [12-14].
A previous study has investigated aminotransferase levels during acute pyelonephritis in adult patients, but such a study has not been performed in children [15]. In the present study, we found that many patients with UTI had elevated aminotransferase levels. The prevalence of increased aminotransferase levels in UTI patients without pre-existing liver disease was approximately 20%.
In the present study, patients with increased aminotransferase levels were younger than those with normal levels. Consequently, clinicians should carefully consider hepatic dysfunction in younger patients with UTI.
A previous study has reported neonatal cholestasis in the context of an UTI [5], but there was no significant increase in total bilirubin level in the present study. Liver dysfunction is not as severe in patients with UTI as in those with cholestasis.
Increased aminotransferase levels have been previously described in approximately 10% of patients treated with cephalosporin [16]. In some cases, this may be due to antimicrobial therapy. However, in the present study there were no significant differences in the regimen of antibiotics.
The changes in aminotransferase levels were mild and self-limiting in this study. In most cases, the levels normalized without the need for any further management during convalescence. We conclude that increased aminotransferase levels during UTI do not require unnecessary tests and excessive treatment.





 XML Download
XML Download