

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastrointestinal congenital anomalies occur in one of every 10,000 neonates. Atresia in the pylorus or prepyroric area comprises less than 1% of those [1]. The most common cause of gastric outlet obstruction for infants up to the age of 3 months is hypertrophic pyloric stenosis [2]. Gerber described the antral membrane as a rare cause of antral and pyloric obstructive deformities [3] that is seen in 1 in 100,000 births [4]. Antral web is a thin fenestrated diaphragm made up of 2 layers of mucosa and usually lacking muscular component [5]. Antral web can be diagnosed in the early infancy, but often is seen even in adults. There are a few sporadic reports in the literature. Herein, we present a case of congenital antral web in premature baby.
CASE REPORT
The baby was born at gestational age of 32+1 weeks with 1,880 g of birth weight and was the 2nd baby of dizygotic twin. His mother was 31-year-old multiparous woman and had no history of polyhydramnios during antenatal exam. After birth, the baby had 3 to 4 times of non-bilious vomiting per day without feeding while meconium passed well. The nature of stool was normal. On physical examination, there was neither abdominal distension nor discoloration.
Laboratory findings at 3 days after birth showed hemoglobin, 19.5 g/dL; hematocrit, 54.8%; white blood cell count, 9,870/mm3 (neutrophils 21.1%); platelet count, 148,000/mm3; and C-reactive protein, 0.03 mg/dL. The biochemical profile consisted of serum protein, 5.6 g/dL; albumin, 3.3 g/dL; total bilirubin, 12.9 mg/dL; direct bilirubin, 1.2 mg/dL; aspartate aminotransferase, 24 U/L; alanine aminotransferase, 4 IU/L; blood urea nitrogen, 16.3 mg/dL; creatinine, 0.68 mg/dL; pH 7.41; sodium 133 mmol/L; potassium 5.9 mmol/L; chloride 100 mmol/L; and total carbon dioxide 18.4 mmol/L.
The infantogram revealed a mild distended stomach with distal small bowel gas. Ultrasonography (USG) results indicated no signs of pylorus hypertrophy or malrotation. The upper gastrointestinal (UGI) series revealed that the stomach was severely distended and the antrum was abruptly narrowed at 1 cm proximal to pylorus. The gastrograffin hardly passed to the pylorus and small bowel (Fig. 1).
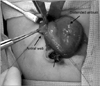
We diagnosed the antral web and performed laparotomy at the 10th day after birth. The stomach was severely distended and the antrum was hypertrophied (Fig. 2). We opened the antrum transversely, and then could find out 2 mm-thick web near pylorus. The 5 Fr feeding tube could not pass the web. The web was excised circumferentially. From antrum to pylorus, Heinecke-Mikulicz pyloroplasty was done to prevent a narrowing of antrum. There was neither intra-operative nor postoperative complication. The baby slowly began milk feeding after 6 postoperative days and eventually reached an intake of 100 mL/kg 20 days after operation. Finally, the baby was discharged at postoperative 35 days with corrected age of 38+4 weeks with body weight 2,420 g.
DISCUSSION
Antral web is a rare cause of congenital gastric outlet obstruction. It is also called mucosal diaphragm of the pyloric antrum or prepyloric diaphragm. Its thickness is usually 2-4 mm and it can be found anywhere from 1 to 7 cm proximal to the pylorus [1]. The etiology of webs remains unknown. The developing mechanism is known to be incomplete recanalization of foregut around gestational age 5-6 weeks [6]. In this period, the epithelial cells rapidly overgrow in the lumen, and vacuoles appear and eventually coalesce to recanalize the gut. The webs may be resulted from an excessive local endodermal proliferation early in gastric development [1,5].
Despite of antral web being a congenital disease, the timing of symptom presentation depends on the size of lumen. In general, lumen sizes larger than 1 cm do not lead to obstructive symptoms [6]. So a few cases of antral web discovered in older children or adults. According to the literature, symptomatic presentation within 10 days postbirth is extremely rare [1-11]. Most patients show intermittent atypical symptoms such as vague abdominal pain, vomiting, or abdominal distension. Some of them show melena or hematemesis [7,8].
In neonate period, there are many causes of non-bilious vomiting such as pyloric stenosis, feeding intolerance, milk allergy, metabolic disorders (e.g., hyperammonemia, metabolic acidosis), increased intracranial pressure, sepsis, necrotizing enterocolitis, or adrenal insufficiency [12]. As shown in our case, we could exclude infectious causes and metabolic disease through physical examination and laboratory findings. Necrotizing enterocolitis is often manifested through increased gastric residue with/without bloody stool after milk feeding. However, non-bilious vomiting even nil per os without abdominal distension gave us an impression of congenital gastric outlet obstruction. We excluded pyloric stenosis, because it is usually apparent after 2 or 3 weeks after birth.
For the diagnosis, USG and UGI series are useful. The conditions causing gastric obstruction on UGI series include prepyloric antral web, pyloric stenosis, pylorospasm, redundant or hypertrophied mucosal folds, perigastric adhesions, or heterotopic pancreatic tissue [4]. For antral web, UGI series reveals persistent, sharp band-like linear defect in antrum and the "double bulb sign". One is normal duodenal bulb and the other one is proximal antral chamber between web and pylorus [10,11,13]. Up to UGI series findings, multiple hypertrophied redundant mucosal folds show usually multiple, more irregular than antral webs and do not encircle the stomach circumferentially [4]. Perigastric adhesions are usually anterior and deform only one wall [4] and ectopic pancreatic tissue has central niche [5]. USG after filling the stomach with milk or saline shows an echogenic diaphragm-like structure in the antrum with gastric dilatation, and delay in gastric emptying with normal pylorus [11]. From endoscopy, we can find the small opening mimicking the pylorus, but it doesn't have a normal mucosal fold, normal peristaltic movement, and cannot close itself [5,8].
However, accurate diagnosis is difficult and often delayed even if the patient undergoes endoscopy or UGI series, because antral web is very rare and does not give an impression to the clinician who doesn't have previous knowledge about it. Patients often have been treated for ulcer or pyloric spasm [8,9]. Asymptomatic antral web become worse from peptic ulcer with edema of antrum [8]. In some cases, the wrong interpretation of UGI series and the partial improvement with H2-blocker may make us believe that the obstruction was the result of chronic peptic ulcer [2].
The symptomatic antral web needs surgical correction [4]. From anatomical lesion, antroplasty or web excision with or without pyloroplasty are possible surgical options [7]. For our patient, the lumen of antrum became very narrow after web excision even though considering for edematous change of antrum. For widening the lumen, we did pyloroplasty. The prognosis is very good after surgical correction [7]. The endoscopic treatment is another option of antral web depending on the feasibility of endoscopic intervention. Endoscopic transection is possible if the the mucosal structure is uniform without major vessels or muscular or serosal layers and the membrane is tense and consistent with perpendicular insertion [6]. However, in our case, endoscopy is impossible to perform in premature baby whose body weight is less than 2 kg.
We suggest that persistent non-bilious vomiting in neonate should be evaluated by USG after excluding possible another causes. Because, antral web is very rare but can cause gastric outlet obstruction from neonatal period. UGI series assuming antral web is important for accurate diagnosis. It can lead early surgical correction with favorable outcome.

 XML Download
XML Download