

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intussusception is not a widely recognized complication of celiac disease. In 1968, Ruoff et al. [1] stated the occurrence of intussusception in adult celiac disease for the first time. An association between adult celiac disease and intussusception has been described. Though more common among children, intussusception has not been linked with childhood celiac disease aside from isolated case reports [2]. For the first time, Germann et al. [3] in 1997 reported celiac disease as an uncommon cause of recurrent intussusception in children. Then Mushtaq et al. [4] reported 3 children with spontaneously resolving small bowel intussusception in association with celiac disease and suggested that the finding of transient small bowel intussusception should have need of prompt investigation for celiac disease. Another 6 cases of intussusception whose initial presentation of celiac disease was reported in pediatric age group in English literature [5-10]. Here, I report two consecutive children with initial presentation of gastrointestinal obstruction due to intussusception, who proved later to have celiac disease.
CASE REPORT
Case 1
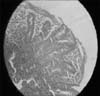
A 7-year-old boy was admitted due to vomiting, diarrhea, and severe abdominal pain since three days ago. His vital signs were stable. In physical examination, he was ill, pale with normal heart and lung. His weight and height were 17 kg (<5% weight percentile for age for boys) and 116 cm (10% height percentile for age). Abdominal examination showed distention, bowel sounds were hyperactive and palpation was painful and tender diffusely without palpable mass. Abdominal ultrasonography was done due to sustained abdominal pain and revealed an intussuscepted bowel segment with pseudo-kidney appearance without obstruction (Fig. 1). His intussusception was reducted neither over the time nor by barium enema, so underwent surgical reduction. Intussusception was ileoileal type, with multiple enlarged lymph nodes. In investigation for concomitant failure to thrive, he was anemic (hemoglobin, 10.4 g/dL) and tissue transglutaminase levels (tTG IgA, IgG) were 268 U/mL (normal range, 0-12), and 3.6 U/mL (normal range, 0-1), respectively. Duodenal biopsies were taken and histopathology revealed marsh III celiac disease (Fig. 2). After 6 months gluten free diet (GFD) his weight raised 3 kg and tTg IgA reached to 28 U/mL and tTG IgG to 1 U/mL.
Case 2
A 5-year-old girl was hospitalized because of abdominal distention and severe bilious vomiting. Her defecation was not changed but was loose. She had history of anorexia, poor weight gain and abdominal distention since infancy but had not have visited previously. She was toxic, febrile and cachectic with weight of 12 kg (<3% weight percentile for age for girls) and height of 96 cm (<5% height percentile for age for girls). Her lung was normal but heart was tachycardic. Abdomen was distended with hyperactive bowel sound, and diffuse tenderness was noted on palpation. Her abdominal X-ray revealed air-fluid levels, indicative of bowel obstruction. Abdominal ultrasonography revealed gas distention of bowel loops and reductable transient intussusceptions with donuts appearance on the right side of the abdomen (Fig. 3). Nasogastric tube was inserted. After three days of serum therapy and administration of antibiotics, vomiting had stopped and abdominal distention decreased gradually. Laboratory tests revealed leukocytosis (18,400/mm3) with polyneucleosis (11,800/mm3), anemia (hemoglobin, 8.4 g/dL), normal serum electrolytes, tTG IgA >800 U/mL, and tTG IgG >200 U/mL. Diagnosis of celiac disease was confirmed with endoscopic duodenal biopsies, showing histopathology of marsh III (Fig. 4). After six months GFD, she had got good appetite and gained 6 kg of weight and her distention was resolved near completely.
DISCUSSION
There are multiple case reports about occurrence and incidence of transient non-obstructive intussusceptions in adult celiac disease [11]. But intussusception as a presenting symptom of pediatric celiac disease has been very rarely reported [2]. Although intussusception is the most common cause of intestinal obstruction in children [12] and celiac disease is a frequent small bowel disease [13], they rarely had been reported in association with each other. In the past decades when barium studies were used more commonly in the diagnosis of malabsorption, transient intussusception was seen in 20% of patients with proven celiac disease [10]. Gonda et al. [14] determined the prevalence of intussusception among a cohort with celiac disease. Of a total of 880 patients, 14 (age 47±17.5 years; 50% female) had intussusception. Intussusception was the initial manifestation of celiac disease in 57% (8/14) and was associated with abdominal pain, but there is no report of intussusceptions after GFD in children. Despite the numerous case reports of intussusception associated celiac disease, Ludvigsson et al. [11] found no association between intussusception and future celiac disease; but mostly modest increased risk of intussusception after diagnosis of celiac disease. Reilly et al. [2] also found that intussusception was far more common among children with untreated celiac disease than in the general pediatric population. Among 254 children with celiac disease, 1.2% experienced the intussusception <9 months before their diagnosis with celiac disease compared with 0.07% of children of their institution in the same time period. They concluded that the diagnosis of celiac disease should be considered in children with intussusception, even in the absence of growth failure.
I report two cases of celiac disease with initial presentation of symptoms of intussusception. Both had growth retardation and were older than usual age of intussusception. The first patient was a 7-year-old slim boy with symptoms of gastroenteritis and severe abdominal pain for three days, in whom abdominal ultrasonography revealed non-obstructive intussusceptions. During surgery, presence of multiple enlarged mesenteric lymph nodes attracted surgeon's attention, the probable cause of intussusception, as others have reported [15]. High level of tTG and duodenal biopsies' histopathology demonstrated celiac disease. The second patient was a thin girl with a distended abdomen and bilious vomiting for two days. Her abdominal ultrasonography showed an invaginated small bowel loop which reducted spontaneously and recurrently. All pediatrics celiac disease records were reviewed in Shahid Motahari Hospital, the only referral pediatric gastrointestinal ward in West Azarbayjan in Iran. The author had documented 41 pediatrics celiac diseases over 6 years, so near 5% of my patients had presented with intussusceptions. The high prevalence of intussusception at Shahid Motahari Hospital maybe associated with small number of our patients, genetic or environmental differences, or awareness to similar subject.
Intussusception can be associated with celiac disease, so that celiac testing is recommended in children with intussusception and growth failure especially in unusual age range.



 XML Download
XML Download