

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastroesophageal reflux (GER) is a physiologic phenomenon, and is defined as the involuntary movement of gastric content into esophagus and is a common phenomenon in infants. Regurgitation is defined as the passage of refluxed contents into the pharynx, mouth, or from the mouth [1], and in inversely related to age [2,3]. If GER persists, it may progress to pathologic GER and become GER-disease (GERD). Non-erosive GERD in the pediatric patient is defined by the presence of troublesome symptoms caused by the reflux of gastric contents and the absence of mucosal breaks at endoscopy [1]. GERD is the result of GER with esophageal mucosa breaks (esophagitis) or complications (anemia, failure to thrive, and hematemesis) [1,4].
In countries with limited financial resources and technical possibilities, like Indonesia, the questionnaire developed by Orenstein et al. [5] and Kleinman et al. [6] may be an important tool to diagnose GERD. According to the data from Orenstein et al. [5] and Kleinman et al. [6], the Infant GER Questionnaire (I-GERQ) and the I-GERQ-revised have a good specificity and positive predictive value in the diagnosis of GERD and justifies the start of empirical treatment, especially in countries where diagnostic possibilities are limited.
Therefore, we studied the natural history of regurgitation and risk to develop GERD in Indonesian infants older than 6 months presenting with regurgitation using the I-GERQ score, the frequency of regurgitation, weight gain and feeding problems during a period of 3 months follow-up.
MATERIALS AND METHODS
A longitudinal prospective survey was conducted during 3 months in 16 Posyandu (a service station for healthy children below 5-year-old, supervised by Primary Health Care Centre) in West Jakarta between September 2012 and February 2013. We included infants aged 6 to 9 months old who regurgitated since more than 2 weeks at least 1 time/day, 4 days/week. The education level of the mother was obtained through a questionnaire: low education (elementary school or primary high school); middle education (senior high school or its equivalent); higher education (Graduated Diploma Degree, Master, PhD), professional education (general practitioners, specialist doctors, pharmacists or its equivalent). The socioeconomic status was classified according to the World Bank 2006 standard, based on per capita income.
We excluded infants with a clinical suspicion of cow milk allergy and infants diagnosed with tuberculosis, neurologic disorders such as spasticity, hypotonicity and cerebral palsy. Other exclusion criteria were severely wasted infants (<3 SD of the "weight to length z-score of the WHO 2006 growth chart"), history of gastrointestinal surgery, history of H2 receptor antagonist or proton pump inhibitor treatment.
The sample size calculation was done based on the formula for single proportion, using the following parameters: estimated prevalence of GERD in the selected group of infants included in the study is 50% (there is no previous publication within this age group), variation of this prevalence (Zα) around 10%, with a confidence interval at 95%. The minimal sample size was calculated at 97 subjects. Anticipation of loss to follow up from previous studies was estimated at 30% [7]. Therefore 130 infants were needed. Hundred thirty-one were included.
The following data were collected from the children that were eligible: birth history, feeding pattern, frequency and estimated volume of regurgitation, position while spitting up, and material that was regurgitated. We also asked for confounding variables such as tobacco exposure, history of GERD (vomiting, heartburn, acid regurgitation and dysphagia) in the family, and history of familial atopy. We collected anthropometric data by measuring body weight (Laica, Barbarano Vicentino, Italy), body length (infantometer provided by Ministry of Health Republic of Indonesia) and head circumference.
The I-GERQ, consisting of 11 questions including frequency and volume of regurgitation, distress during regurgitation, feeding refusal, weight gain, crying or fussiness, hiccups, arching back, apnea or cyanosis [5,6]. The questionnaire has been linguistically validated (translation to Indonesian language, backward translation, and conceptual equivalence). The I-GERQ has a maximal score of 25. According to the data published by Orenstein et al. [5], a score>7 was considered as suggestive for GERD. All participants with a score>7 were referred to the Cipto Mangunkusumo Hospital for further investigation. If the score was ≤7, the child was seen again the next month, and this during 3 consecutive months. In patients with frequent feeding (>8 times/day) or if the ingested volume was estimated excessive, parental education consisted of avoiding excessive feeding volumes and reducing increased frequency of feeding to normal for the age of the infant. Advice was given to adapt the position of the baby during and after feeding, by holding the baby in vertical position for 30-45 minutes. All data were analyzed with SPSS Statistics version 17.0 (SPSS Inc., Chicago, IL, USA).
The study was approved by the Ethics Committee of the Faculty of Medicine, University of Indonesia: 558A/PT02.FK/ETIK/2012 (approved on 18 September 2012). An informed consent was obtained from one of the parents.
RESULTS
Infant characteristics
Hundred thirty-one infants were enrolled in this study; 4 infants were lost to follow-up and only 1 infant had a I-GERQ score of >7 and was diagnosed with GERD. The majority of the infants was 6 months old and had normal anthropometric parameters. Maternal education level was low-middle in 96.9%, and economic status was low (53.4%) and middle (43.5%). The socio-economic status was low (57.2%), middle (41.2%; 54/131), and high (1.5%). The characteristics of the included infants are shown in Table 1.
Most of the infants regurgitated 3 or more times/day and spit up an estimated volume of more than 15 mL. The frequency and volume of regurgitation decreased during follow-up. At the end of follow-up, there was no infant who regurgitated more than once a day, more than 4 days/week and or large volume of regurgitation (15 mL; Table 2).
The median value of the I-GERQ score at study entry was 4 (3-7). In most of the infants, two questions determined the level of the score: "weight gain problems" and "hiccups more than normal" (Table 3). Eighty-five parents were educated regarding frequency of feeding. If the parents were asked for "the most common position in which the baby did regurgitate", they answered the upright position in 49.6%, prone position in 37.4%, and in supine in 13%. We also advised the parents to keep their infant in the vertical position for 30-45 minutes after each feeding. Regurgitation could be related with the postprandial phase or was not related with feeding, in 52.7% and 47.3%, respectively. Milk was by far the most frequent regurgitated food (79.4%) followed by saliva (20.6%). We educated the parents not to give breast or formula milk before or after solid food.
An evaluation of this non-pharmacologic therapy was performed in the next follow-up. There were only 6 infants that still had frequent regurgitation (>3 times/day) despite an appropriate feeding schedule. Of the 91 parents that were informed about feeding schedules and position, 4 were lost to follow-up.
The I-GERQ score reached a score of 0 in 50% of the infants after one month of follow-up, in 64.3% and in 81.9% at the second and third month of follow-up (Fig. 1). Twenty-two infants still regurgitated at the end of the follow-up period; 2 of them were 12 months old. After 1 month of follow-up, 1 infant (0.7%) had developed an I-GERQ score of 8 and met GERD diagnostic criteria. This infant was 10 months old and presented with regurgitation 3-5 times/day, with an estimated volume of 15-30 mL, feeding refusal and insufficient weight gain.
Factors that related with regurgitation that persisted after 3 months follow-up
Considering the risk factors for persistence of regurgitation, we did a bivariate and multivariate analysis for sex, age, exclusively breastfeeding, smoke exposure, family history of GER, and non-pharmacotherapy. No significant difference was found for any of these variables in bivariate or multivariate analysis (Tables 4 and 5). Twenty-two infants still regurgitated >3 times/day after 3 months follow-up; 3 infants among the 22 (14%) had complied with non-pharmacotherapy education, whereas 19 infants among the 22 (86%) infants that still regurgitated at the end of follow-up did not comply with the educational advice given.
Weight gaining and feeding matters
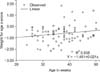
The weight gain of all infants during the 3 months follow-up was 755.8±503.9 gram (confidence interval [CI] 95% 667-844.7). Mean difference of weight to age z-score in infants with persistence of regurgitation compared with those in whom regurgitation ceased at the end of the 3 months follow-up were -0.006±0.357 (95% CI, -0,164-0,152), p=0.939 and 0.108±0.530 (95% CI, 0.005-0.211), p=0.041. The trends of the z-score in these two groups of infants are shown in Figs. 2 and 3.
After 3 months follow-up, there were still feeding problems in 19 infants. Feeding problems identified in this study included feeding refusal, feeding time of more than 1 hour, or parent reported that they felt "upset" during mealtime. Seventeen infants among 19 infants had an I-GERQ score 0 at the end of follow-up. Thus 17 out of 19 infants with feeding problems did not regurgitate.
DISCUSSION
Regurgitation is a very common physiologic event in infants under 6 months of age. Nelson et al. [3] reported that "at least 1 episode of regurgitation per day" reaches a peak at the age of 4 months (67% of all infants), decreases to 21% in 6-7 months old infants and reaches 6% in 10-12 months old infants. Martin et al. [7] reported a similar prevalence of regurgitation in Australian infants reaching its peak at the age of 3-4 months (41%), decreasing to 35% in 6-7 months old infants, 15% in 8-9 months old infants, and 10% in 10-11 months old infants, respectively. Publications from Japan and Thailand by Miyazawa et al. [8] and Osatakul et al. [9] showed a similar pattern. A previous study from Indonesia by Hegar et al. [10] showed a peak of regurgitation at the age of 4 months (68.6%), decreasing to 35.7% in 4 to 8 months old infants.
According to the data from Hegar et al. [10], Indonesian infants only seldom regurgitate more than 4 times/day after the age of 8 months. After the age of 6-7 months, regurgitation decreases because of several developmental factors. Infants also start to have solid food.
In Italy, Campanozzi et al. [11] used a modified I-GERQ, studying 313 healthy infants presenting with regurgitation at least 2 times/day (Rome II criteria). After 24 months of follow-up, 1 subject (0.5%) was diagnosed with GERD. The I-GERQ score reached 0 in 27%, 61%, 11%, and 1% of the subjects after 6, 12, 18 and 24 months follow-up [11]. Van Howe and Storms [12] in Michigan followed prospectively a cohort of 128 1-month old infants during 6 month. Using the I-GERQ-Revised questionnaire, GERD was found in 25.5% (95% CI, 16.7-34.4), 12.5% (95% CI, 5.9-19.1), 8% (95% CI, 3.7-13.3), 2.9% (95% CI, 0-6.2) infants aged 1, 2, 4, and 6 months, respectively [12].
De et al. [13] used also used the I-GERQ to investigate GERD at a tertiary health care hospital in North India. They studied 612 infants and excluded subjects with a severe acute illness. GERD was found in 10% of the subjects (61/602) and most of them (44.6%) in the age group of 1-6 month, 25% in the group that was 6-12 months old, and 30.4% in the group that was 12-24 months old [13].
In our study, we did not find a significant difference in variables that may interfere with persistent regurgitation. Breast milk may be a protective factor because it enhances gastric emptying, and because regurgitation and vomiting are symptoms of cow's milk protein allergy, which is 5 to 10 times more frequent in formula fed than in breastfed infants [4,14]. But, Martin, Miyazawa, and Osatakul did not find a relation between exclusive breastfeeding and regurgitation [7-9]. Campanozzi et al. [11] found at inclusion that exclusively breastfed infants did statistically not regurgitate less than formula fed infants; however, the I-GER-Q reached 0 earlier in exclusively breastfed infants than in formula fed infants, 8.2±3.9 months vs 9.6±4.1 months (p=0.03).
All studies (Martin et al. [7], Hegar et al. [10], Campanozzi et al. [11], and Van Howe and Storms [12]) confirm the absence of an association between exposure to tobacco smoke and regurgitation.
History of atopy in family members may be associated with regurgitation, especially in cow milk allergy cases [15], but we had excluded suspicion of cow milk allergy at enrollment. Martin et al. [7] did report that infants regurgitating longer than 90 days during their first year of life had an odds ratio of 1.6 (95% CI, 1.1-2.3) to have a mother with at least 1 symptom of GER and an odds ratio of 1.5 (95% CI, 1.1-2.1) to have a mother without symptom of GER.
Non-pharmacotherapy through reassurance and feeding advice has been strongly recommended by North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and European Society for Pediatric Gastroenterology, Hepatology, and Nutrition as the first step in the therapeutic approach [14]. Hegar et al. [16] showed that parental reassurance remains the cornerstone of treatment of regurgitation. Shalaby and Orenstein [17] showed that conservative treatment (feeding modification, restricting the volume, and positioning) was effective even via a telephone contact in 24% of a cohort of infants that was suspected of GERD. In our study, reassurance and non-pharmacologic treatment showed around a 50% better outcome than no intervention (20.4 versus 9%, respectively).
Interestingly we found an increase of the "weight for age z-score" trends in infants that still regurgitated at the end of follow-up and a declining z-score in infants that no longer regurgitated. This finding is in line with the findings of Campanozzi [11], Miyazawa et al. [8], and Osatakul et al. [9] which showed that there is no weight gain problem in infants presenting with regurgitation. An explanation may be that infants that regurgitate drink larger volumes than infants who do not regurgitate. Unfortunately, we did not register the volumes that the infants ingested. Overfeeding is always postulated as a reason for infant regurgitation; however, data confirming this are missing.
Feeding problems are frequently reported in infants with physiologic GER [18]. Infants with regurgitation have a 4.2 times (95% CI, 1.4-12.0) increased risk to have feeding problems compared to controls [15]. Behavioral and feeding problems are common in all infants; feeding problems were reported in 25-50% of healthy infants [15,19]. Nelson et al. [20] stated that the etiology of feeding problems at this age is multifactorial.
In conclusion, GERD is a rare condition in infants older than 6 months that regurgitate at least once a day. Our study suggests that the efficacy of a non-pharmacologic therapeutic approach is successful and that regurgitation resolves commonly through increasing age. We did find a relationship between regurgitation and weight gain, weight gain being greater in regurgitating than in non-regurgitating infants. The hypothesis that larger feeding volumes may be responsible for this finding needs to be further investigated.







 XML Download
XML Download