

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute urinary retention is infrequent in children. The most common causes of acute urinary retention of children are neurological process, severe voiding dysfunction, urinary tract infection, adverse drug effects and constipation [1]. Acute urinary retention in constipation is caused by anterior displacement of the bladder base and trigone by the stool-filled rectum, impairing urethrovesical and sacral reflex function [2]. Fecaloma is an accumulation of inspissated feces in the colon or rectum, giving the appearance of an abdominal tumor which is much harder than a fecal impaction [3]. Herein, we report a 47-month-old girl presented with acute urinary retention caused by a giant fecaloma in the reformed septum after Duhamel procedure for Hirschsprung disease.
CASE REPORT
Past medical history
The patient was born fullterm with a birth weight of 2.4 kg. At the age of 2 weeks, she was diagnosed with Hirschsprung disease and underwent the Duhamel operation. At that time, a ganglion cell was noted at the proximal sigmoid. After the operation, she was able to evacuate the bowels well until 6 months of age and she stopped visiting the outpatient clinic. She has a history of constipation of over 1 year. Constipation had been managed with oral lactulose and enema using glycerin at a nearby hospital over 1 year when she complained abdominal pain, agitation and holding her stools with 3- or 4-day interval. After enema, sausage-shaped stools were frequently observed. Her mother could not remember the exact characters of stool. There was no abnormal and unusual feeding history or urinary pattern before admission.
Present illness
The patient was transferred to our hospital due to acute urinary obstruction. One week ago, diffuse lower abdominal pain developed which was managed at a local clinic with medicine for constipation. However, abdominal pain persisted. One day before admission, abdominal distension and voiding difficulty developed.
Physical examination
On initial evaluation the patient had a blood pressure of 110/70 mmHg, a pulse rate of 96 beats/min, a respiratory rate of 24 breaths/min, a body temperature of 36.5℃ with a body weight of 14.5 kg (the 50-75 percentile) and a height 99.9 cm (>the 97 percentile). She was irritable because she could not pass urine despite the feeling of micturition. Her abdomen was distended, and focal tenderness was present at the lower quadrant. Auscultation revealed lower than normal bowel sounds. The location of the anal orifice on the perineal area and anal tone were both physiologic. No abnormal dimple or skin lesion on her sacral area was observed and her neurologic examination was physiologic and normal. Fecal materials were palpable on digital rectal examination.
Radiologic and laboratory findings
Abundant fecal materials were observed on abdominal X-ray (Fig. 1), and ultrasonography (USG) of the abdomen revealed a distended bladder with a thin bladder wall and both hydronephrosis of grade III (Fig. 2). Hematological examinations and blood chemistries were as follows: a hemoglobin level of 13.0 g/dL, a total white cell count of 5.9×109/L, a platelet count of 357×109/L and granulocyte and lymphocyte levels of 41.5% and 46.1%, respectively; A serum calcium level of 9.7 mg/dL (8.6-10.2), a magnesium level of 1.2 mg/dL (1.5-2.3), a sodium level of 144.1 mmol/L (135-145), a potassium level of 3.6 mmol/L (3.3-5.1) and a chloride level of 104.6 mmol/L (98-110). Her blood urea nitrogen, creatinine, hepatic transaminase and C-reactive protein levels were normal. Urinalysis collected via a catheter was normal. Thyroid function test was not checked. Sigmoidoscopy could not be performed to her because of a large amount of feces in her distal colon despite repeated glycerin enema and digital evacuation.
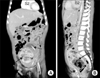
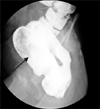
Hospital course
After urinary catheterization, 720 mL of urine was drained and abdominal pain and distension was improved. However, urinary obstruction persisted and urinary catheterization was kept continuously. On day 3 after admission, voiding difficulty persisted despite loose stool passage after repeated glycerine enema. For ruled out the abdominal mass, whole-abdominal computed tomography (CT) was performed and showed a large fecaloma in the sigmoid colon and a displaced bladder (Fig. 3). The coronal image of the CT showed that the distal part of the colon was markedly dilated and contained heterogeneous materials consisting of impacted feces. The markedly dilated distal colon was suspected as Duhamel pouch. The bladder neck was displaced into the upper abdomen because of the large fecaloma-filled pouch. After repeated glycerin enemas and digital evacuations, spontaneous urination was noted on day 5. USG revealed a normal sized bladder and improved both hydronephrosis. However, she could not evacuate bowels sufficiently by herself. We could palpate a membranous tissue in her rectum at the time of digital evacuation. On day 7, a colon study revealed a giant Duhamel pouch filled with fecal materials without a definitive the membranous tissue in her rectum (Fig. 4). We decided to perform an operation because she had a giant Duhamel pouch, an unidentified membranous tissue and to perform a full-thickness rectal biopsy. Two weeks later, operation was done after sufficient evacuation of the feces in her rectum. A septum was noted in Duhamel pouch, which ran transverse direction in her rectum on the operative findings. Post-Duhamel septum revision was performed. Histopathologic findings of the full-thickness rectal biopsies showed a ganglion cell in the rectum. Since the operation, she has been visiting our outpatient clinic regularly. She has been free of defecation and urination difficulties without the need for medicine.
DISCUSSION
Common complications after repair of Hischsprung disease are obstruction, fecal incontinence and enterocolitis. The outcome after Swensen, Duhamel and Soave procedures for Hirschsprung disease is similar. However, the Duhamel procedure is known to have less risk of overall complications except the risk of postoperative enterocolitis. Constipation and fecal impactions as obstructive symptoms are common complications of Duhamel operation and mega Duhamel pouch [4] as in this case.
When obstructive symptoms after repair of Hirschsprung disease are present, the possibility of anatomic and functional problems should be considered. In our case, stenosis of the anastomotic site and anus were ruled out by digital rectal examination and colon study. In order to differentiate between acquired and secondary aganglionosis following the pull-through procedure and neuronal intestinal dysplasia, a full-thickness rectal biopsy was performed during operation, which revealed a normal appearing-ganglion cell in her remaining colon. Persistent internal anal sphincter (IAS) dysfunction is another cause of obstructive symptoms after repair of Hirschsprung disease and is related to specific abnormalities in IAS innervations [5]. The patient might have had IAS dysfunction but her obstructive symptoms were improved after post-Duhamel septum revision without myectomy or sphincter-diving procedure. Even though her obstructive symptoms were improved, regular follow-up and anorectal manometry are warranted.
There could be several causes for reoperation after the Duhamel procedure such as bleeding, leakage and stenosis [6,7]. Septum formation after the Duhamel procedure is one of the stenotic causes for reoperation [6,7]. Most patients with fecaloma including our case have a long history of constipation. In our patient, the septum might have aggravated fecaloma formation, causing medicine to be less effective.
Causes of fecaloma have been described in association with Hirschsprung disease [8], Chagas disease [9], both inflammatory and neoplastic disease, and in patients suffering with chronic constipation [3]. Fecaloma was the presenting symptom of Hirschprung disease in a 5 month-old male in China [8]. Inversely, the megacolon was the result of fecaloma in an older child [10] and an adult [11]. In addition, fecaloma formation is the most common complication after the Duhamel operation [5]. However, no child with Hirschsprung disease has shown clinical urologic problems after rectosigmoidectomy and Duhamel-type pull-through procedure [12]. Constipation accounts for 25% of the visits to the pediatric gastroenterologist [13] and is commonly associated with an overactive bladder rather than acute urinary retention [8]. Urinary symptoms with constipation are urge incontinence, urinary tract infection, frequency, nocturia, holding maneuvers, and enuresis [14]. Hydronephrosis with a large fecal impaction has been reported [15-19] but acute urinary obstruction is not common in children. In our case, the massively distended Duhamel pouch and rectum filled her pelvic cavity and pressed up against the posterior aspect of the bladder and its neck. Fecaloma and secondary acute urinary retention were due to delayed detection of the septum because of discontinuation of visits to the outpatient clinic soon after the first surgery.
Fecalomas can be extracted using laxatives, enemas and rectal evacuation while others require treatment with colostomy [20]. In our case, fecaloma was not completely resolved by repeated digital evacuation and laxatives because of the rectal septum. Thus, she was required to undergo reoperation.
Remaining rectal septum is one of the causes for the reoperation of Hirschsprung disease. In early detection of the septum, there might be no difficult procedure and no need to suffer from longstanding constipation secondary to the septum, in our case. This present case suggests that regular follow-up for evaluation of complications is important for patient who underwent the Duhamel operation.
Moreover, fecaloma should be considered in the differential diagnosis of patients with acute urinary retention especially in those a long history of constipation or the Duhamel operation.


 XML Download
XML Download