

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
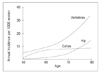
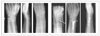
Estrogen deficiency causes a severe dysfunction in the bone homeostasis and bone resorption. Because of the wide surface area of cancellous bone, the primary bone loss occurs at the bony trabeculae of cancellous bone. Resorption pits on the surface of the trabeculae also play an important role in the development of fragility fracture as a stress riser. Since the vertebral body and distal radius have a high proportion of cancellous bone, fragility fractures during menopause are usually vertebral fracture and Colles' fracture. Surgical correction of these fractures is sometimes indicated in this age group. When surgical intervention is indicated, an anatomical restoration of the fracture is essential because of the high social activity and long life expectancy in these patients. A collapse of the vertebral body causes bending of the spinal column and shifting of the weight bearing line. It also causes abnormal stress on the adjacent vertebral body and subsequent vertebral fracture. The rationale of the surgical treatment is to control the acute pain from the fracture and to restore the mechanical axis of the spinal column. Stretching of the hand is a protective mechanism of the fall, which decreases the impacting force on the hip joint, while it frequently causes Colles' fracture on the wrist. During the past few decades, it has been thought as a benign injury, which does not cause any dysfunction. Now orthopaedic surgeons are requested to restore the function of the upper extremity as well as the anatomy of the joint.
Figures and Tables



References
1. van der Linden JC, Homminga J, Verhaar JA, Weinans H. Mechanical consequences of bone loss in cancellous bone. J Bone Miner Res. 2001. 16:457–465.

3. Ahn YH. Internal fixation in osteoporotic bone. 2002. New York: Thieme;9–21.
4. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001. 285:785–795.
6. Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR. Study of Osteoporotic Fracture Research Group. Vertebral fractures and mortality in older women: A prospective study. Arch Intern Med. 1999. 159:1215–1220.
7. Parfitt AM. Implications of architecture for the pathogenesis and prevention of vertebral fracture. Bone. 1992. 13:Suppl 2. S41–S47.
8. Watts NB, Harris ST, Genant HK. Treatment of painful osteoporotic vertebral fractures with percutaneous vertebroplasty or kyphoplasty. Osteoporos Int. 2001. 12:429–437.
9. Mehbod A, Aunoble S, Le Huec JC. Vertebroplasty for osteoporotic spine fracture: prevention and treatment. Eur Spine J. 2003. 12:S155–S162.
10. Kaneda K, Asano S, Hashimoto T. The treatment of osteoporotic-posttraumatic vertebral collapse using the Kaneda device and a bioactive ceramic vertebral prosthesis. Spine. 1992. 17:S295–S303.
11. Hammerberg KW, DeWald RL. Senile burst fracture: a complication of osteoporosis. Orthop Trans. 1989. 13:97.
12. Young BT, Rayan GM. Outcome following nonoperative treatment of displaced distal radius fracture in low-demand patients older than 60 years. J Hand Surg Am. 2000. 25:19–28.
13. Ring D, Prommersberger KJ, Gonzalez del Pino J, Capomassi M, slulitel M, Jupiter JB. Corrective osteotomy for intra-articular malunion of the distal part of the radius. J Bone Joint Surg. 2005. 87-A:1503–1509.
14. Paul MS, Andrew JW. Fractures of the distal aspect of the radius: Changes in treatment over the past two decades. Instr Course Lect. 2003. 52:185–195.
15. Katz MA, Beredjiklian PK, Bozentka DJ, Steinberg DR. Computed tomography scanning of intra-articular distal radius fractures : Does it influence treatment? J Hand Surg Am. 2004. 26:415–421.
16. Jakob M, Rikli D, Regazzoni P. Fractures of the distal radius treated by internal fixation and early function. J Bone Joint Surg Br. 2000. 82:340–344.
17. Gupta R, Bozentka DJ, Osterman AL. Wrist arthroscopy: Principles and clinical applications. J Am Acad Orthop Surg. 2001. 9:200–209.
20. Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin endocrinol Metab. 2005. 90:1294–1301.
21. Cao Y, Mori S, Mashiba T, Westmore MS, Ma L, Norimatsu H, et al. Raloxifene, estrogen, and alendronate affect the processes of fracture repair differently in ovariectomized rats. J Bone Miner Res. 2002. 17:2237–2246.
22. Mashiba T, Turner CH, Hirano T, Forwood MR, Johnston CC, Burr DB. Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone. 2001. 28:524–531.
23. Bouxsein ML, Kaufman J, Tosi L, Cummings S, Lane J, Johnell O. Recommendations for optimal care of the fragility fracture patient to reduce the risk of future fracture. J Am Acad Orthop Surg. 2004. 12:385–395. (Korean edition).
 XML Download
XML Download