

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
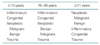
For the differential diagnosis of head and neck mass lesions, the age and presenting locations should be the primary considerations. The characteristic patterns of age- and site-predilection allow a diagnostic work-up and treatment plans for the patients with head and neck mass lesions. In children and young adults, the underlying causes are; inflammatory, congenital and developmental, and neoplastic masses in decreasing frequency. By contrast, neoplastic diseases are most frequent in the elderly. Because of the characteristic lymphatic spread patterns of head and neck diseases, the location of the mass in the cervical lymphatic nodal chain may be the key for the identification and differential diagnosis of the primary disease site. Besides, the evaluation of specific historical and physical findings is mandatory for the accurate diagnosis. When the signs of inflammation are associated, conservative treatment and observation is first considered. On the other hand, for persistent or progressively enlarging masses and those with suspicious findings of malignancy, surgical intervention should be considered.
Figures and Tables





References
2. McGuit WF. Shockley WW, Pillsbury HC, editors. Neck Masses: Differential Diagnosis and Therapeutic Approach. THE NECK Diagnosis and Surgery. 1994. St. Louis: Mosby-Year Book;73–89.
3. Altman RP, Margileth AM. Cervical lymphadenopathy from atypical mycobacteria: Diagnosis and surgical treatment. J Pediatr Surg. 1975. 10:411–417.
4. Coker DD, Casterline PF, Chambers RG, Jaques DA. Metastases to lymph nodes of the head and neck from an unknown primary site. Am J Surg. 1977. 134:517–522.

5. Lee D-J, Rostock RA, Harris A, Kashima H, Johns M. Clinical evaluation of patients with occult primary tumor. South Med J. 1986. 79:979–983.
6. Lindberg R. Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tract. Cancer. 1972. 29:1446–1449.
7. Knight PJ, Mulne AF, Vassy LE. When is lymph node biopsy indicated in children with enlarged peripheral nodes? Pediatrics. 1982. 69:391–396.
8. DeVita VT Jr, Jaffe ES, Hellman S. DeVita VT, Hellman S, Rosenberg SA, editors. Hodgkin's disease and the non-Hodgkin's lymphomas. Cancer. Principles and Practice of Oncology. 1985. 2nd ed. Philadelphia: JB Lippincott Co;1623–1710.
9. Skandalakis JE, Godwin JT, Androulakis JA, Gray SW. The differential diagnosis of tumors of the neck. Prog Clin cancer. 1970. 4:141–159.
10. MacComb WS. Diagnosis and treatment of metastatic cervical cancerous nodes from unknown primary site. Am J Surg. 1972. 124:441–449.
11. Parsons JT, Million RR, Cassisi NJ. The influence of excisional or incisional biopsy of metastatic neck nodes on the management of head and neck cancer. Int J Radiat Oncol Biol Phys. 1985. 11:1447–1454.
12. Shapiro AL, Pincus RL. Fine needle aspiration of diffuse cervical lymphadenopathy in patients with acquired immunodeficiency syndrome. Otolaryngol Head Neck Surg. 1991. 105:419–421.
13. McGuirt WF. Panendoscopy as a screening examination for simultaneous primary tumors in head and neck cancer: A prospective sequential study and review of the literature. Laryngoscope. 1982. 92:569–576.
14. Drake AF, Hulka GF. Shockley WW, Pillsbury HC, editors. Congenital Neck Masses. THE NECK Diagnosis and Surgery. 1994. St. Louis: Mosby-Year Book;93–107.
15. Sistrunk WE. Technique of removal of cysts and sinuses of the thyroglossal duct. Surg Gynecol Obstet. 1928. 46:109.
16. Maddox PR, Malcolm HW. Clark OH, Duh QY, Kebebew E, editors. Approach to thyroid nodules. Textbook of Endocrine Surgery. 2005. 2nd ed. Philadelphia: Elsevier Saunders;85–92.
17. Fujimoto Y, Obara T, Okamoto T. Clark OH, Duh QY, Kebebew E, editors. Papillary thyroid carcinoma: Rationale for hemithyroidectomy. Textbook of Endocrine Surgery. 2005. 2nd ed. Philadelphia: Elsevier Saunders;102–109.
18. Clark OH. Clark OH, Duh QY, Kebebew E, editors. Papillary thyroid carcinoma: Rationale for total thyroidectomy. Textbook of Endocrine Surgery. 2005. 2nd ed. Philadelphia: Elsevier Saunders;110–113.
19. Hamming JF, Roukema JA. Clark OH, Duh QY, Kebebew E, editors. Management of regional lymph nodes in papullary, follicular, and medullary thyroid cancer. Textbook of Endocrine Surgery. 2005. 2nd ed. Philadelphia: Elsevier Saunders;195–206.
21. Moley JF, Shervin N. Clark OH, Duh QY, Kebebew E, editors. Medullary thyroid carcinoma. Textbook of Endocrine Surgery. 2005. 2nd ed. Philadelphia: Elsevier Saunders;129–141.
 XML Download
XML Download