

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Timely diagnosis and subsequent appropriate intervention is important in respiratory diseases. Chest radiograph is the most commonly performed radiologic examination and is the imaging study that the majority of non-radiologist physicians are most likely to encounter in their clinical practice. Chest radiography, however, can be very complex and difficult to interpret accurately due to abnormalities that might be quite subtle. Failure to detect lung cancer on the chest radiograph, which has become one of the most frequent causes of missed diagnoses in radiology, is a major cause that brings up medicolegal suits. There are no reliable radiographic criteria to distinguish lung cancer from benign diseases. Being knowledgeable about thoracic imaging will help to minimize errors. The diagnosis of lung cancer is commonly delayed because of masking by a tuberculosis lesion. In diagnosing tuberculosis, clinicians should be aware of endobronchial tuberculosis, anthracofibrosis, multidrug resistant tuberculosis, and non-tuberculous mycobacterial diseases. If pneumonia was not resolved, endobronchial lesions such as a foreign body or cancer, bronchioloalveolar cell carcinoma, and atypical pathogens might be considered. In patients with chronic coughing, eosinophilic bronchitis also should be suspected in addition to postnasal drip syndrome, cough variant asthma, and gastroesophageal reflux disease. Most common pitfalls can be avoided by physicians who are familiar with diverse patterns of respiratory disease in diagnosis. Through an increased familiarity with variable manifestations of pulmonary diseases and a high index of suspicion, the diagnosis of respiratory diseases will be improved.
Figures and Tables
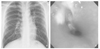
Figure 1
A forty-five-old male lung cancer patient who was delayed diagnosed for several months because of normal chest radiograph
A) Chest radiograph shows no definite abnormality, B) Photograph of bronchoscopy in the carina reveals a large tumor mass, C) On CT scan of chest, narrowed both main bronchus with large tumor mass

Figure 2
A twenty-two old male endobronchial tuberculosis patient who was treated as bronchial asthma for several months before admission
A) Chest radiograph shows no definite abnormality, B) The bronchoscopic photograph in the right upper lobe bronchus shows hyperemic dirty mucosa covered with actively caseating tuberculous lesion

References
1. Midtun DE, Jett JR. Clinical presentation of lung cancer, Lung Cancer, Principle and Practice. 1996. 2nd ed. Philadelphia: Linppincott-Raven;421–437.
2. Irwin RS, Widdicomde GF. Cough, Textbook of Respiratory Medicine. 2000. 3rd ed. Philadelphia: Sounders;553–556.
4. Woodring JH. Pitfalls in the radiologic diagnosis of lung cancer. AJR. 1990. 154:1165–1175.

5. Kim YI, Goo JM, KIM HY, Song JW, Im JG. Coexisting bronchogenic carcinoma on the chest radiography in clinical practice: radiologic findings and clinical significance. Korean J Radiol. 2001. 2:138–144.
6. Stitik FP, Tockman MS. Radiolographic screening in the early detection of lung cancer. Radiol Clin North Am. 1978. 16:347–366.
7. Austin JH, Romney BM, Goldsmith LS. Missed bronchogenic carcinoma: radiographic findings in 27 patients with a potentially resectable lesion evident in retrospect. Radiology. 1992. 182:115–122.
8. Muhm JR, Miller WE, Fontana RS, Sander DR, Uhlenhopp MA. Lung cancer detected during a screening program using four-month chest radiographs. Radiology. 1983. 148:609–615.
9. Lam SC, Palcic B. Fluorescence Detection, Lung Cancer. 2nd ed. Blackwell Science;269–286.
10. David O, Alan MF, Steven HF. The solitary pulmonary nodule. N Engl J Med. 2003. 348:2535–2542.
11. Ting YM, Church WR, Ravikishnan KP. Lung carcinoma superimposed on pulmonary tuberculosis. Radiology. 1976. 119:307–312.
15. Kern KA. Medicolegal analysis of the delayed diagnosis of cancer in 338 cases in the United States. Arch Surg. 1994. 129:397–403.
17. Chung MP, Lee KS, Han J, Rhee CH, Han YC, Kwon OJ. Bronchial stenosis due to anthracofibrosis. Chest. 1998. 113:344–350.
20. Barkley JE, Green MR. Bronchioloalveolar carcinoma. J Clin Oncol. 1996. 14:2377–2386.
22. Cassiere H, Rodrigues JC, Fein AM. Delayed resolution of pneumonia. When is slow healing too slow? Postgrad Med. 1996. 99:151–154. 157–158.
23. Joo JH, Park SJ, Park SW, Lee JH, Kim DJ, Park CS, et al. Clinical features of eosinophilic bronchitis. Korean J Intern Med. 2002. 17:31–37.
 XML Download
XML Download