

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The treatment of malignant tumors of the pelvic bone has been considered difficult. Many authors have reported lower rates of patients survival and high rates of complications after treatment of the malignant bone tumors of the pelvis. The size of the tumors often much greater than in other sites. Surgical resection and reconstruction often are more complex, based on the proximity of neurovascular structures. Resection of the tumor varies widely in size, type and location of the lesion. After resection of the tumor, reconstruction restoring anatomy of the pelvis and hip, maintaining the limb length and retaining function of the hip joint are challenging procedures. Reconstructions depend on extent and types of resection, type I(iliac). type II(periacetabular) and type III(pubic or ischial) and combined resection. Although limb salvage procedures are advisable in most of patients, there are times when external hemipelvectomy should be considered the treatment of choice. If surgical margin is not safe, or if major neurovascular structures are sacrificed for the wide resection, and consequently residual limbs are functionless, external hemipelvectomy should be considered. Once limb salvage surgery with resection is chosen as the most appropriate treatment for the patient, careful decision should be made whether reconstruction is necessary and what type of reconstruction is necessary. Most of type I resection could be reconstructed with sacroiliac arthrodesis with a recycled autograft or allograft. The vascularized bone graft may be augmented. Type II resections could be reconstructed with saddle prosthesis or recycled autograft with prosthesis composite. Type III resections are usually not necessary for reconstruction due to little functional impairment. However, most of type I, II combined resection and type I, II, III combined resection are almost impossible to solid reconstruction, and are not advisable to reconstruction. At times, it is appropriate to leave patients with a pseudarthrosis. Reconstruction should be individualized by types and extent of resection.
Figures and Tables
 | Figure 1Types of pelvic resections
Type I: Iliac resection, Type II: Periacetabular resection, Type III: Pubic resection
|
 | Figure 2A 38 year old male patient who had a chondrosarcoma at his Right ilium(A), was treated with wide resection and reconstruction with non-vascularized fibular graft and bridging plates and screws. At one year follow up, the patient showed good functional result with satisfaction (B).
|
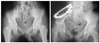
 | Figure 3Pelvis AP radiograph of a 40 year old female showed radiolucent destructive bony lesion in right ischium(A,B). Incisional biopsy revealed chondrosarcoma. The patient was managed with wide resection and reconstruction with saddle prosthesis(C). At 7 year and 6 month follow up, she showed well maintained prosthesis with excellent functional result(97% of normal)(D).
|
 | Figure 4A pelvis AP radiograph of a 68 year old male showed radiolucent bony lesion in left ilium, periacetabulum and upper part of ischium(A). Bone scan revealed a hot uptake(B) and MRI demonstrated extent of involvement(C). Incisional biopsy revealed chondrosarcoma. He was managed with type I+II+III pelvic resection without any reconstruction(D). Ten months after operation he showed relatively goodfunctional result(57% of normal) without any evidence of remained disease.
|
References
1. Wilkins RM, Cullen JW, Camozzi AB, Jamroz BA, Odom L. Improved survival in primary npn-metastatic pediatric osteosarcoma of the extremity. Clin Orthop. 2005. 438:128–136.
2. Kang Y, Lee H, Koh H, Rhyu K, Song J, Choi J. Functional results after limb salvage surgery for osteosarcoma. J Korean Bone Joint Tumor Soc. 1998. 4:199–205.
3. Chung Y, Rhee S, Kim H, Bahk W, Lee A, Kang Y, et al. Clinical outcome of stage IIB osteosarcomas in long bones. J Korean Bone Joint Tumor Soc. 2006. 12(1):1–7.
4. Saab R, Rao BN, Rodriguez-Galindo C, Billups CA, Fortenberry TN, Daw NC. Osteosarcoma of the pelvis in children and young adults: The St. Jude children's research hospital experience. Cancer. 2005. 103(7):1468–1474.

5. Shin K, Rougraff BT, Simon MA. Oncological outcome of primary bone sarcomas of the pelvis. Clin Orthop. 1994. 304:207–217.
6. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM. Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer. 1996. 78:745–750.
7. Kawai A, Huvos A, Meyers PA, Healey JH. Osteosarcoma of the pelvis: Oncological results of 40 patients. Clin Orthop. 1998. 348:196–207.
8. Bell RS, Davis AM, Wunder JS, Buconjic T, McGovern B, Gross AE. Allograft reconstruction of the acetabulum after resection of Stage II-B sarcoma. J bone Joint Surg Am. 1998. 80:1396–1397.
9. Mankin H, Hornicek FJ, Temple HT, Gebhardt MC. Malignant tumors of the pelvis. Clin Orthop. 2004. 425:212–217.
10. Wirbel RJ, Schulte M, Mutschler WE. Surgical treatment of pelvic sarcomas. Clin Orthop. 2001. 390:190–205.
11. Hillmann A, Hoffmann C, Gosheger G, Rodl R, Winkelmann W, Ozaki T. Tumors of the pelvis: complications after reconstruction. Arch Orthop Trauma surg. 2003. 123:340–344.
12. Hugate R, Sim FH. Pelvic reconstruction techniques. Orthop Clin N Am. 2006. 37:85–97.
13. Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg. 1978. 60A:731–746.
14. Campanacci M, Capanna R. Pelvic resections: The Rizzoli Institute experience. Orthop Clin North Am. 1991. 22:65–86.
15. Abudu A, Grimer RJ. Reconstruction of the hemipelvis after the excision of malignant tumors. J Bone Joint Surg[Br]. 1997. 79-B:773–779.
16. Ozaki T, Hillmann A, Lindner N, Blasius S, Winkelmann W. Chondrosarcoma of the pelvis. Clin Orthop. 1997. 337:226–239.
 XML Download
XML Download