

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervix cancer is one of the leading causes of cancer related morbidity worldwide and the fourth leading cause of death in women [1]. The incidence and death due to cervix cancer is declining in developed countries with the introduction of cervical screening and the introduction of vaccination programs. These measures have only been introduced recently and cervix cancer will continue to remain a significant health problem in marginalised communities and countries without such programs [1].
The current standard of chemoradiotherapy (CCRT) and brachytherapy (BT) for the treatment of cervix cancer is based on studies where majority of patients were less than 70 years of age [23]. Recently published results of radiotherapy treatment of cervix cancer patients from our institute reported a 5-year relapse-free survival (RFS) and overall survival (OS) of 66% and 65%, respectively [4]. The mean age in this patient cohort was 58 years.
With increasing life span, elderly population is expected to increase in future [5]. Individuals aged 65 or more are anticipated to reach 19% of the population in USA by 2030 [6]. Elderly patients are a heterogeneous group with respect to performance status, comorbidities, access to healthcare and motivation to participate in screening programs [7]. These factors may be associated with the delayed diagnosis of cervix cancer in this population and treatment could be further compromised due to the perceived decreased ability to tolerate, accept or be considered for complex treatment [8]. Management decisions therefore need to be highly individualised [9].
There is limited data on the patterns of care, treatment toxicity, and the outcomes in elderly patients with cervix cancer. Additionally, the information about age-related factors that could potentially influence the treatment outcomes would be useful in guiding management decisions.
The aim of this study was to determine the management patterns of elderly cervix cancer patients referred for radiotherapy as well as to report the RFS in the patients treated with curative intent. Secondary aims were to investigate the treatment tolerability as measured by treatment related toxicities and the appropriateness of patient selection for curative and palliative radiotherapy.
MATERIALS AND METHODS
All patients referred to the Peter MacCallum Cancer Centre (PMCC) Gynaecology Radiation Oncology unit with a diagnosis of cervix carcinoma were prospectively entered into an ethics-approved tumour registry.
1. Patient selection and assessment
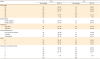
Patients aged ≥75 years and above diagnosed with previously untreated cervix cancer who presented to PMCC between January 1998 and December 2010 for radiotherapy as part of their treatment (either definitive or adjuvant postoperative radiotherapy) were eligible for the study. Patients with known metastatic disease upon initial presentation, or referred for disease recurrence were excluded. All patients were clinically staged using the International Federation of Gynecology and Obstetrics (FIGO) staging criteria. Patients’ baseline Eastern Cooperative Oncology Group (ECOG) performance status and comorbidities were also recorded and utilised to generate a modified Charlson comorbidity index (CCI) [10]. Patients being considered for curative treatment underwent magnetic resonance imaging (MRI) to assess the local extent of disease and position emission tomography-computed tomography (PET-CT) or PET for nodal staging and to exclude distant metastasis. Of 126 patients that met eligibility criteria, MRI was performed in 97 patients and PET was done in 85 patients. Generally, MRI and PET information was not used to change clinical FIGO staging, except where MRI and PET findings would put patients in stage 4b category. Within the 4b category, patients were eligible for this analysis provided all known disease was able to be encompassed within the pelvic field, including metastasis or direct invasion into pelvic bone only or disease involving inguinal nodes. Baseline characteristics of patients are described in Table 1.
Table 1
Patient baseline characteristics

2. Treatment
All patients received external beam radiotherapy (EBRT) as adjuvant (n=10), definitive (n=81), or palliative hypofractionated regimen (n=35). Definitive and adjuvant radiotherapy technique have been previously described [41112]. Briefly, EBRT consisted of a four-field technique with 18 MV photons. Adjuvant radiotherapy consisted of 45 to 54 Gy of EBRT. Definitive radiotherapy consisted of 40 to 45 Gy of EBRT followed by BT. BT was given with either tandem and ovoids (T&O) or tandem and cylinder. EBRT was given with concurrent weekly cisplatin (40 mg/m2) or carboplatin (area under curve (AUC) 2) in the majority of patients, unless contraindicated, as shown in Tables 2, 3. Lymph node (LN) negative patients and patients with metastatic nodes confined to the pelvis were treated with pelvic fields in prone position on a belly board. The upper border of pelvic field was at L5–S1. The patients with common iliac or para-aortic (PA) nodes were treated supine with 4-field extended field radiotherapy (EFRT). The upper border of the PA field was kept 4 cm above the upper most involved node. Involved nodes received a rectangular nodal boosts dose of 6 to 10 Gy in 2 Gy fractions.
Table 2
Use of concurrent chemotherapy in patients treated with curative intent

| Radiotherapy treatment | Cisplatin (40 mg/m2) | Carboplatin (AUC 2) | No chemotherapy |
|---|---|---|---|
| Definitive EBRT (n=81) | 33 | 31 | 17 |
| Adjuvant radiotherapy (n=10) | 4 | 3 | 3 |
Table 3
Reasons for receiving carboplatin or no concurrent chemotherapy
| Variable | No. | |
|---|---|---|
| Carboplatin | 34 | |
| ECOG/comorbidities | 9 | |
| Hearing impairment | 10 | |
| Neuropathy | 3 | |
| Renal function | 12 | |
| No chemotherapy | 20 | |
| Patient preference | 9 | |
| Other (age/ECOG) | 11 | |
Of the 35 patients treated with palliative intent, radiotherapy consisted of a series of 1–3 the so-called “quad-shots” (QSs) [13]. Each QS consisted of 14 Gy in four fractions separated by 4 weeks interval without the use of concurrent chemotherapy. Where suitable, patients also received BT following EBRT. Radiation effectiveness of single QS (given in four fractions) in 2 Gy fraction equivalent radiation dose (EQD2) was 15.8 Gy for acute effects (tumour tissue) and 18.2 Gy for late effects [14]. Those receiving 3 QS (EQD2=47.3 Gy acute and 54.6 Gy late effect) to the pelvis and with the addition of two BT received EQD2 of approximately 78 Gy to the primary tumour volume [14].
Thirteen patients received three QS followed by BT, whilst one patient following pelvic surgery for a rectal cancer was treated with BT alone without the EBRT. Patients with disease limited to pelvis were treated with three QS and BT, provided their ECOG performance status was adequate. The remaining patients who were deemed unsuitable either by treating physician due to performance status or patient refusal of more radical therapy, received 1–2 QS EBRT followed by 1–2 BT or just QS EBRT (1–3) only.
3. Follow-up
All patients were reviewed 4 to 6 weeks postcompletion of radiotherapy and thereafter every 3 to 4 months for the first 3 years, every 6 months for the fourth and fifth years and annually until 10 years. A posttreatment PET or PET-CT was performed 6 months after completion of curative RT to assess response to treatment. Follow-up information about disease status and late complications were prospectively collected. Late treatment-related toxicities were scored according to modified World Health Organization/Radiation Therapy Oncology Group criteria. Once the disease recurrence was confirmed, patients were treated with radiotherapy, systemic chemotherapy or best supportive care as appropriate. Date and cause of death, if known, were documented.
Patient follow-up data was censored at 1st Aug 2012, as it was the earliest of the last follow-up date among those who were alive and not lost to follow-up.
4. Criteria for assessing outcomes
Failure was defined as either persistent disease following radiotherapy or recurrence of disease. The date of failure was taken as the date of sign of any failure. Sites of failure were recorded as: (1) local: residual or recurrent disease at cervix or uterus; (2) pelvic: all failures below L5–S1 including nodal, parametrial, and vaginal; (3) abdominal: PA nodes above L5–S1; and/or (4) distant: including supraclavicular, and inguinal and systemic spread. For first failure at multiple sites, the dominant site of failure was determined according to the hierarchy, in descending order: distant, abdominal, pelvic, and local.
5. Statistical methods
Patient characteristics were described using descriptive statistics. OS was defined as the duration of time between the date of diagnosis and the date of death from any cause; RFS was defined as the duration of time between date of diagnosis and date of first failure. Kaplan-Meier survival curves were calculated for OS and RFS. Times to events were censored by the closeout date. Prognostic factors for OS and RFS were evaluated using Cox proportional hazards regression models. Moreover, subgroup analyses were performed stratified by treatment intent. Treatment toxicities were expressed as proportions.
RESULTS
1. Patient characteristics
There were 194 eligible patients based on FIGO staging criteria. Fifty-two patients had disease beyond the PA nodes and 16 patients had small cell and clear cell histology. These were excluded. The analysis was restricted to the remaining 126 patients, of these, 113 were squamous cell carcinoma (SCC) and 13 had adenocarcinoma histology.
The median follow-up time was 37 months (interquartile range, 10.5 to 71.1 months). All observations were censored on the 1st August 2012. Three patients were lost to follow-up at 6 and 7 years and one patient at 125 days from the date of their histological diagnosis.
The mean age was 81.5 years (SD, 4.6 years) and ranged from 75 to 98. The FIGO stage 1, 2, and 3&4 (as a single group) was estimated in 26%, 41%, and 28% respectively. Ninety-one patients were treated with curative intent and 35 patients received palliative radiotherapy. There were statistically significant (p<0.05) differences in most of the characteristics between the patients treated with curative intent and those treated with palliative intent.
2. Relapse-free survival and overall survival
At the closeout date, 20 of the 21 patients were alive and had no evidence of disease and 102 patients had died. Of those who died, 43% died from other causes without any relapse of cervix cancer, 44% died of disease and three patients were lost to follow-up. Only one of 35 patients treated with palliative intent was alive at 5 years without any evidence of disease.
OS of the entire cohort of patients at 3 years was 52.7% (95% CI, 43 to 61) and at 5 years was 41.2% (95% CI, 32 to 49). RFS at 3 years was 62.88% (95% CI, 53 to 70) and at 5 years was 59.51% (95% CI, 49 to 67).
Ninety-one patients were treated with curative intent. OS in this group at 3 years was 66.63% (95% CI, 55 to 75) and at 5 years was 54.48% (95% CI, 43 to 64). RFS at 3 years was 75.86% (95% CI, 65 to 83) and at 5 years was 71.57% (95% CI, 60 to 80) (Fig. 1). RFS at 3 years according to various prognostic factors are described in Table 4.
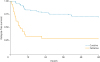
Table 4
RFS and OS at 3 years in patients treated with curative intent
Thirteen of 35 patients who received hypofractionated (palliative) radiotherapy remained disease free in the pelvis until last follow-up or death. Five patients survived for 7.5, 7, 6, 5, and 4 years respectively without any evidence of disease. All five patients were node-negative and were staged as either FIGO stage 1b or 2a. The remaining eight died of unrelated causes whilst one died of distant metastasis at 3 years without any signs of locoregional disease (Table 5, cause of death).

3. Treatment toxicities
Nearly all patients treated with CCRT with curative intent completed treatment. Thirty-five percent of patients treated with CCRT experienced a drop in their hemoglobin below 120 g/L. Two patients required a treatment break due to acute toxicity. One patient had intractable diarrhoea but subsequently completed treatment after a short break. The other patient developed neutropenic sepsis and subsequently died of uncontrolled sepsis. Late toxicity details are shown in Table 6. Half the number of patients remained completely asymptomatic. None of the patients had grade 4 toxicity.
Table 6
Treatment related late toxicity
4. Patterns of failure in patients treated with curative intent (n=91)
Twenty-four (26%) of 91 patients experienced relapse of their disease. Failure rates for primary, pelvis, and PA and distant sites were 7%, 7%, 16%, and 16% respectively. Only one patient with FIGO stage 3b failed exclusively at the primary site. All other failures were multisite. The failure rate in patients with positive nodes was 44%. The failure rate in node negative patient was 24%.
DISCUSSION
To our knowledge, this is one of the largest series of prospectively collected dataset of elderly cervix cancer patients treated with adequate follow-up. The age of 75 years and above was selected based on the published definition as “elderly” in cancer literature [8151617].
The prognosis of cervix cancer in elderly was reported to be inferior in comparison to younger patients. This was thought to be due to increased risk of cancer mortality and treatment related complications in this population [81518]. However, this has not been a consistent finding [192021]. This discrepancy could be due to the heterogeneous patient population of varying performance status, comorbidity, emotional, and social factors as well as personal belief and attitude of treating physician towards elderly [22]. In general, patient’s performance status and comorbidity not only influences patients’ allocation to a particular treatment protocol, but also exert a direct effect on survival due to other causes [23]. In the present study, we found ECOG performance status a better indicator in predicting patient outcome and tolerability of treatment than comorbidity score, measured by CCI. While ECOG status and CCI scores generally did not relate with each other, patients who were excluded from curative treatment in favour of palliative radiotherapy group tended to have higher CCI score and poorer ECOG performance status. Each unit increase in ECOG score increased the risk death by 1.69-fold (p<0.001).
In addition, our data suggests that elderly patients also benefited from BT even in palliative setting. We have found advanced age alone did not influence the efficacy or the ability to tolerate BT. BT should be considered whenever possible [22].
Elderly patients may present with advanced stage disease. This could be due to a combination of factors including stoic tendencies, or have disease that remained relatively asymptomatic relative to comorbidity, disability, and geriatric syndromes [24]. In the current series the proportion of patients presented with FIGO stage 1b, 2, and 3&4 was 26%, 45%, and 28%. There was a marginal difference in stage frequency when compared with the corresponding stages of disease at presentation in age-unrestricted cohort published earlier, where the corresponding proportions were 30%, 50%, and 20%. Similarly corpus-invasive disease was noted in 68% patients as compared with 63% in age unrestricted series [425]. However, metastatic LN were observed in 22% patients which was lower than those found in age-unrestricted series where the corresponding figure was 48% [4]. The failure rate in patients with positive nodes was 44% which is similar to node-positive in the age unrestricted group. The failure rate in node-negative patient was 24%, which was marginally higher than 20% in the age unrestricted series.
Five-year RFS of 71% in this patient population treated with curative intent is regarded as an excellent result. This was possible due to appropriate patient selection based on radiological imaging. Moreover, 80% of patients treated with curative intent in this series were stage 1 and 2. The incidence of metastatic LN in cervix cancer up to FIGO stage 2B has been well documented in surgical series whereby metastatic LN were found in 22% patients with predominantly FIGO stage 1 disease [26] and up to 35% to 40% in stage 2 disease [27]. In the present series, 27% patients in curative group had metastatic LNs. However due to selection bias, patients with stage 3 or more (51%) and greater metastatic LN burden (60%) were shifted to palliative group. This selection of patients has most likely contributed to higher survival in curatively treated patients.
Although RFS in this age group was acceptable at 3 and 5 years, the corresponding OS figures of 66.63% and 54.48% was lower in comparison to the age-matched controls in the previously published series. The average life expectancy for an 82-year-old woman is 7.8 years [28]. One of the main contributing factors for reduced OS has been due to the death by age related factors, as demonstrated in Table 6 where 38 out of 67 patients treated curatively died due to non-disease related causes.
Twenty-six percent patients treated curatively experienced relapse of their disease. The corresponding figure in the age unrestricted series published earlier was 34% [4]. This was likely due to the lower incidence of LNs metastasis at 22% in this series, compared to 48% observed in the earlier series. Similarly the patterns of failure, local, nodal and distant were not dissimilar at 7%, 23%, and16% respectively compared with 13%, 27%, and 21% in age unrestricted cervix cancer patient population [4]. Although the trend from local to nodal and distant failure is similar, the differences can be explained by the fact that many more patients in the elderly population tended to die from age related illness and did not survive sufficiently long to clinically manifest their recurrences.
Sixty percent of patients who were alive and disease free remained completely asymptomatic. There was no grade 4 toxicity observed. Grade 2 and 3 bowel toxicity was observed each in 6% patients. Grade 2, bladder toxicity was observed in 5% with no incidence of reported grade 3 toxicity. Unfortunately 29% patients experienced grade 2 or 3 vaginal toxicity, which was higher than the younger cohort of patients in our institute [429]. This was due to non-compliance and lack of motivation in using vaginal cylinder and oestrogen cream. The disease behaviour, tolerability of CCRT with BT and treatment outcome in appropriately selected elderly cervix cancer patients was comparable to age unrestricted patient population. This finding is consistent with other published studies [2230].
Palliative RT resulted in good symptoms and disease control. Early stage, node negative patients appear to have been cured using this less demanding hypofractionated regimen. A shorter course of low dose palliative radiotherapy was appropriate for advanced FIGO stage patients with poor performance status, comorbidities and/or extrapelvic metastatic nodal disease who would likely fail both within and outside radiation field despite a protracted course of curative radiotherapy. The selection of palliative treatment by treating physician was arrived at in consultation with the patient and their relatives in light of perceived poor tolerability of curative CCRT. The majority of patients treated with palliative intent were ECOG status 3, CCI ≥3, or had metastatic nodes up to the upper PA region.
Thirteen of 35 patients who received hypofractionated radiotherapy remained disease-free. Eleven of these patients were node negative and two had presented with positive nodes. All patients who presented with FIGO stage 3b and above (n=15) had relapsed. The one who survived at 6 years was 86 years old, had stage 2a disease with SCC histology and inferior PA node, was treated with single QS to EFRT and later converted to fractionated radiotherapy and two T&O. Eighty per cent of the 18 patients with stage 3 (n=9) and 4 (n=9) disease had metastatic LN. Of the LN-positive patients 75% had PA nodes. All except one died within 18 months of their diagnosis, most within a year of multi-site failures. The patient who was >4 years disease-free and died of unrelated cause was 80 years old, had stage 3a SCC cervix with inferior PA node, was treated with only two QS without any BT.
In terms of late toxicity, 21 patients (60%) did not report any symptoms and nor had any evidence of toxicities on clinical examination. Five of these were disease-free and long-term survivors. However, only a third of these patients were alive for more than 1 year following their diagnosis. The rest died with multisite failure within 14 months of their diagnosis. Only one patient had grade 3, bowel toxicity. This was a patient with metastatic PA node and had received one QS to EFRT and later converted to fractionated radiotherapy and two T&O. She was alive and diseases free at 6 years until the last follow-up. Another patient who had stage 3b disease and received three QS without BT developed vaginal fistula continuous with uterine cavity with residual tumour at the primary site and pelvic nodes. Although documented as vaginal toxicity, this was caused by the cavity left by the resolving tumour and regrowth of tumour in radiated tissue. It is likely that low rate of late toxicity following hypofractionated radiotherapy could be related to limited survival in these elderly patients.
In conclusion, radiotherapy for cervix cancer in the elderly population is well tolerated. Hypofractionated regimens with or without BT are a suitable alternative for low risk disease in patients not fit for radical treatment. Patient selection is of utmost importance in order to tailor appropriate management in elderly individuals.
 XML Download
XML Download