

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) is the most common and one of the most lethal gynecologic malignancies worldwide [1], with a particularly high incidence in developed countries [2]. Although there has been progress in its primary treatment [345], EOC is widely known for its poor prognosis and high recurrence rate, with 22% percent of EOC patients experiencing recurrence within six months of primary therapy [6]. Complete cytoreductive surgery followed by chemotherapy is generally accepted as the standard treatment for primary EOC, though its role in recurrent EOC is not as clear. However, a number of studies have shown that complete debulking of the tumor during secondary cytoreductive surgery is an independent prognostic factor for improved survival [78910].
Recently, laparoscopy has replaced laparotomy in a number of surgeries for gynecologic cancer due to improvements in techniques and instrument quality. The laparoscopic approach has been commonly used in the treatment of cervical cancer and endometrial cancer [1112]. Laparoscopy has advantages such as a better visual field, less blood loss, fewer postoperative adhesions, less need for analgesics for postoperative pain control, fewer hospital days, and faster onset of adjuvant therapy due to fast recovery. There have been successful attempts in using the laparoscopic approach to manage early-stage EOC [1314]. However, the use of the laparoscopic approach in recurrent EOC management is still controversial.
There are currently on-going trials investigating the efficacy of chemotherapy and/or angiogenesis inhibitor in recurrent EOC after secondary cytoreduction (Gynecology Oncology Group 213). In addition, the results from a large ongoing RCT (DESKTOP III) comparing the efficacy of chemotherapy and cytoreductive surgery in recurrent EOC will soon be available. Although there are still debates on whether secondary cytoreduction is optimal management for recurrent EOC, current National Comprehensive Cancer Network (NCCN) guidelines for EOC suggest the consideration of secondary cytoreductive surgery in platinum-sensitive tumors with radiographic relapse. If cytoreduction has a role in the treatment of recurrent EOC, laparoscopy could be considered as an option. In this study, we evaluated the feasibility of laparoscopic cytoreduction in selected patients with localized recurrent EOC by investigating surgical outcomes and survival.
MATERIALS AND METHODS
We performed a retrospective review of all patients with EOC who underwent an operation at Samsung Medical Center during the period between January 2002 and December 2013. Data were abstracted from the patient electronic medical records. The study was approved by Institutional Review Board of Samsung Medical Center (file no. 2014-12-064).
1. Patients
During the retrospective chart review, the following inclusion criteria for this study were applied: (1) an attempted secondary cytoreduction after a diagnosis of recurrence; (2) disease-free interval (DFI) ≥12 months; (3) good performance status before surgery as defined by Eastern Cooperative Oncology Group (ECOG; performance status 0–2); (4) localized single recurrence pattern without ascites by preoperative imaging studies. In selecting the patients for secondary cytoreduction in recurrent EOC, the inclusion criteria were set based on those published in major retrospective studies [151617181920].
Patients with a localized single recurrence and no ascites were considered candidates for this study. Localized recurrence was defined as recurrence limited within the pelvis, upper abdomen, or mid-abdomen without apparent intraperitoneal dissemination by imaging studies such as computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography-CT scan. We defined an isolated pattern as up to three nodules at a single recurrent site or lesion. DFI was defined as the period after the initial primary debulking surgery (PDS) until the time of recurrence.
The flowchart of patient selection is shown in Fig. 1. Of the 879 patients with EOC treated at Samsung Medical Center from January 2002 to December 2013, patients who were not optimized after PDS were excluded. In addition, only patients with recurrence (n=403) were included. After applying the inclusion criteria, 79 patients were determined to be appropriate candidates for the current study. Patients were divided into two groups according to surgical method. None of the candidates had received chemotherapy prior to their cytoreduction for recurrence.

2. Oncological assessment
Both surgical groups were compared according to patient demographics, surgical characteristics, and surgical outcomes. Procedures related to the removal of recurrent lesions (peritoneal nodule resection/peritonectomy, lymphadenectomy, omental nodule resection/omentectomy, hepatic segmentectomy, splenectomy, low anterior resection, hemicolectomy, segmental resection of colon, segmental resection of small bowel) and the repair of injuries (ureteral stenting, vessel, and bowel primary repair) during the secondary cytoreduction were described. For most of the laparoscopic procedures, a transumbilical approach was used with 3 to 4 ancillary trocars placed in the abdomen according to the location of the suspected recurrent lesions. A rigid 5 or 10 mm scope was used for laparoscopy. The removal of the specimen during the laparoscopic procedure was usually performed through the site of scope insertion with the specimens removed in an endoscopic bag. With larger specimens such as those removed from splenectomy or hepatic segmentectomy, an additional incision using a previous operation scar or an enlargement of a trocar incision was used for removal. Complete versus incomplete debulking was defined according to the presence of a visible tumor of any size at the completion of surgery. After secondary cytoreduction, patients were routinely evaluated with imaging studies (abdominopelvic CT or MRI) for confirmation of complete cytoreduction. Operating time was measured from the beginning of skin incision to the completion of skin closure. Blood loss was estimated by the difference in the total amounts of suctioned and irrigated fluids. An estimated amount of blood loss based on the number of gauze and lap pads used during the procedure was calculated in laparotomy patients. Follow-up after secondary cytoreduction was performed as follows. After treatment, patients were assessed by physical examination, complete blood count, and chemistry with serum tumor markers including cancer antigen 125 (CA-125) measurements every 3 months for the first 2 years and twice per year thereafter; chest radiography and abdominopelvic CT scan (or alternatively abdominopelvic MRI) were performed every 6 months for the first 3 years and every 12 months; thereafter, additional diagnostic procedures were performed according to specific clinical suspicions. For survival analysis, we defined progression-free survival (PFS) as the period from the time of secondary cytoreduction with/without chemotherapy to relapse or the final follow-up visit; overall survival (OS) was the period from the time of secondary cytoreduction with/without chemotherapy to death or the final follow-up visit.
3. Statistical analysis
Summary statistics were used to describe the data. Values are presented as median (range) for continuous variables, and frequencies (percentages) for categorical variables. Baseline clinical characteristics and study outcomes were compared between the two age groups using the Mann-Whitney test for continuous variables, and the chi-square test or Fisher exact test for categorical variables, as appropriate. The Kaplan-Meier method was used to estimate PFS and OS. Statistical analyses were performed using IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA). A two-sided p<0.05 was considered statistically significant.
RESULTS
1. Patient characteristics/surgical characteristics
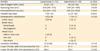
Demographic data and surgical characteristics for both surgical groups are shown in Tables 1, 2. There were no statistically significant differences between the two groups of patients in terms of age, body mass index, CA-125 level, tumor type, initial stage, or grade. The peritoneal surface appeared to be the most frequent site of recurrence. Differences in the type of procedures and the adjuvant treatment after secondary cytoreduction were not associated with statistical significance. Most of the surgical procedures were related to the removal of recurrent disease. Multiple procedures were largely performed to repair intraoperative complications such as ureter, vessel, or bowel injury. Chemotherapeutic agents mostly consisted of carboplatin/paclitaxel. Chemotherapy schedules were determined according to the surgeon’s preference with consideration of factors such as patient status and previous toxicity. The difference in the median DFI of the two groups was statistically insignificant (p=0.752).
Table 1
Patient demographics by surgical group
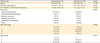
Table 2
Surgical characteristics of two surgical groups in recurrent epithelial ovarian cancer

2. Surgical outcomes
Table 3 lists the surgical outcomes of the two groups. The results showed significantly shorter median operation time (100 minutes vs. 140 minutes, p=0.026) and median hospital days (7 days vs. 11 days, p<0.001) in laparoscopy group. In addition, less estimated blood loss was observed in the laparoscopy group than in the laparotomy group (100 mL vs. 200 mL, respectively; p=0.003). Intraoperative complications occurred in four cases (12.8%) from the laparoscopy group and in seven cases (14.7%) from the laparotomy group. In the laparoscopy group, intraoperative complications were mostly due to ureter injury, while injuries to various locations including the bowel, ureter, and vessels were observed in the laparotomy group. Complete debulking was achieved in all cases from the laparoscopy group and in 95.8% of cases from the laparotomy group. Given the median follow-up time of 35 months (range, 2 to 119 months), the differences between the two groups in the 5-year PFS rate and OS rate after secondary cytoreduction were not statistically significant, as shown in Table 3 (p=0.252 and p=0.262).
Table 3
Surgical outcomes of two surgical groups in recurrent epithelial ovarian cancer
DISCUSSION
To the best of our knowledge, this is one of the largest series comparing laparoscopy and laparotomy in secondary cytoreduction for EOC patients with a localized recurrence pattern. Although the standard treatment for recurrent ovarian cancer has not been clearly defined, previous studies have demonstrated that secondary cytoreduction has a clinical benefit for patients with localized recurrence [21]. One recent report compared minimally invasive technique and laparotomy [20] and demonstrated that a laparoscopic approach had a clinical benefit in patients with isolated recurrence. This study is a continuation of these previous studies and was intended to provide additional information about the surgical outcomes of the two different approaches.
Our results showed that a laparoscopic approach in patients with recurrent EOC can be a successful treatment option without increased morbidity and with acceptable survival. In the laparoscopy group, less blood loss, shorter operating times, and shorter hospital stays were demonstrated. Complete debulking was achieved in all cases of laparoscopy. According to previous studies of minimally invasive surgical approaches in secondary or tertiary cytoreduction, the rates of optimal cytoreduction were 81.8% to 96.2% [192022]. In our cohort, the optimal rate of 100% was achieved in the laparoscopy group. A high rate of complete cytoreduction may be achieved by careful selection of the surgical candidates. Imaging studies prior to secondary cytoreduction play a very important role in this selection process. The careful effort in patient selection with preoperative imaging evaluations may have led to excellent results.
Given the difficulties in palpating abdominal structures as well as directly visualizing the abdominal cavity with laparoscopy, preoperative evaluation is important in selecting the patients suitable for a minimally invasive approach. With recent improvements in the quality of radiologic evaluations, we tried to preoperatively predict the presence of multiple adhesions or fibrosis. In the near future, we may be able to use intraoperative ultrasound or narrow-band imaging to assess the intraabdominal environment, provided these methods are sufficiently validated [2324].
This study has limitations due to its retrospective nature. In retrospectively selecting the surgical approach of the patients, differences between the two groups affecting survival outcomes could exist even though the same inclusion criteria were applied. Surgeons may have selected laparoscopy for patients with smaller-sized recurrence, as differences in the size of the recurrent lesions appeared in the data. However, this study mainly focused on perioperative outcomes. We could conclude that laparoscopy is feasible in cases of recurrent EOC on a limited basis. However, the observation period was not long enough to gain adequate information for survival analyses. In addition, a study with a larger number of patients may be needed in the future to validate our results.
EOC is known as a fatal disease and the prognosis is even worse with relapse. In addition to survival, quality of life should be considered as an important factor in the treatment of patients with recurrent EOC. With this perspective, less invasive surgery offers several perioperative advantages over laparotomy if it does not compromise survival. In addition, the faster recovery from less invasive surgery allows patients to start adjuvant chemotherapy earlier than patients recovering from laparotomy.
In conclusion, the laparoscopic approach can be feasible option for the treatment of recurrent EOC, with benefits that include less blood loss, shorter operating time, and shorter hospital stays. In EOC patients with a localized single recurrence site, laparoscopy can be performed safely without compromising patient outcomes or morbidity.
 XML Download
XML Download