

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prognostic factors in endometrial cancer include surgical stage, histological subtype, histological grade, lymph node (LN) metastasis, peritoneal cytology, lympho-vascular space invasion (LVSI), myometrial invasion, cervical involvement, and extrauterine disease [1,2]. Based on these factors, the postoperative recurrence risk of endometrial cancer is classified into low-, intermediate-, and high-risk groups [3]. Although patients with low-risk endometrial cancer do not benefit from pelvic lymphadenectomy [4,5], those with high-risk endometrial cancer may benefit from combined pelvic and para-aortic lymphadenectomy [678]. Several reports have also suggested that patients with intermediate-risk endometrial cancer benefit from lymphadenectomy [78910]. Patients with intermediate-risk disease in whom no LN metastasis is detected by routine microscopic examination may have occult microscopic disease in their LNs.
In the field of breast cancer, because sentinel LN biopsy has been a standard procedure worldwide for more than 10 years, several studies concerning small tumor deposits in regional LNs have been published [1112131415]. Detailed examination of sentinel nodes by serial sectioning and immunohistochemical staining can result in the detection of extremely small tumors [16]. The Cancer Staging Manual of the American Joint Committee on Cancer defines isolated tumor cells (ITC) as tumor cell clusters that are ≤0.2 mm at the largest diameter, denoted as pN0 [i+]; whereas micrometastases (MM) are defined as those that are >0.2 mm in diameter but ≤2 mm, denoted as pN1mi [17]. It was initially reported that the presence of ITC or MM is not an adverse prognostic factor in breast cancer. In 2009, Hansen et al. [11] reported that the 8-year overall and disease-free survival of patients with negative nodal status, ITC, or MM were not significantly different. They concluded that patients with ITC or MM do not have a worse prognosis than node-negative patients. However, they also showed that patients with ITC or MM underwent adjuvant chemotherapy and axillary LN dissection more often than node-negative patients. Conversely, de Boer et al. [12] assessed a large amount of data from the Netherlands Cancer Registry and found that early-stage breast cancer patients with ITC or MM in regional LNs who had not received adjuvant therapy had a reduced 5-year disease-free survival rate. They also performed a meta-analysis that showed that the presence of metastases of ≤2 mm in regional LNs is associated with poor survival [13]. Andersson et al. [14] reported that MM have a negative impact on survival whereas ITC do not. However, they also found that patients with ITC underwent axillary LN dissection significantly more often than those with no detected LN deposits. Leidenius et al. [15] reported that the presence of ITC is an adverse prognostic factor in early breast cancer. These reports suggest that small tumor deposits have a negative impact on survival; however, the difference in survival between ITC or MM and node-negative cases is small and might be eliminated by adjuvant treatment.
Although some reports on the clinical significance of sentinel node mapping in endometrial cancer have recently been published, sentinel LN biopsy is not a standard procedure for endometrial cancer. At present, therefore, gynecological oncologists rarely identify patients with ITC or MM in their LNs. However, the issue of treatment of patients with ITC or MM will arise in the near future because it is highly possible that the opportunity for physicians to perform ultrastaging of sentinel LNs will increase. In the field of endometrial cancer, few studies have compared the survival outcomes of patients with ITC or MM in their LNs and node-negative patients. In the present study, we attempted to make this comparison.
MATERIALS AND METHODS
1. Study subjects
Approval by the Institutional Review Board was obtained from the Ethics Boards of Hokkaido Cancer Center on June 2012. A retrospective search of patient records identified 260 patients with malignant tumors of the uterine corpus who had been treated in the Division of Gynecology of Hokkaido Cancer Center from 1997 to 2004. Twenty-eight patients with uterine sarcoma/carcinosarcoma were excluded from the analysis. Of the 232 patients with endometrial carcinoma, 55 had undergone surgery without lymphadenectomy, and five had not undergone any surgery. Hence, 172 patients had undergone extensive surgical staging, including lymphadenectomy.
In this study, categorization of risk grouping was based on the 2008 International Federation of Gynecology and Obstetrics (FIGO) staging system, tumor grade, histological subtype, LVSI, and peritoneal cytology. Patients with FIGO stages III and IV disease were classified as high risk, those with FIGO stage IA with endometrioid G1/G2 tumor, no LVSI, and negative peritoneal cytology were classified as low risk, and all other tumors were classified as intermediate risk. In other words, intermediate risk was defined as having at least one of the following factors: (1) >50% myomerial invasion; (2) grade 3 disease or non-endometrioid histology; (3) cervical involvement; (4) LVSI; and (5) positive peritoneal cytology. Of the 172 patients who underwent appropriate surgical staging, 30 were high-risk and 79 were low-risk endometrial cancer. A total of 63 patients with intermediate-risk endometrial cancer were enrolled in this study.
2. Ultrastaging of lymph node micrometastasis
Ultrastaging involving multiple slicing, staining, and examination of specimens was performed on 2,475 LNs that had been diagnosed as negative for metastases to assess the presence of microscopic tumor cells, including ITCs. Because no paraffin-embedded blocks were available for two patients, ultrastaging was performed in 61 patients.
Our method of ultrastaging was reported in a previous paper [18]. The slicing process consisted of cutting five pairs of 4-μm-thick serial sections (10 sections in total) from archival, formalin-fixed, paraffin-embedded blocks containing all resected LNs. Pairs of serial sections were cut at 120-μm intervals. Four hundred twenty-four paraffin-embedded blocks were examined, each containing several LNs. A total of 4,240 sections were prepared.
The staining process consisted of hematoxylin and eosin (H&E) staining of one section and AE1/AE3 monoclonal antibody staining (Nichirei, Tokyo, Japan) of the other section from each pair (2,120 sections were stained with H&E and 2,120 with cytokeratin). Staining was performed using an automated immunostainer (NexES, Ventana, Tucson, AZ, USA). Microscopic tumors were classified as ITC (≤0.2 mm in diameter) or MM (0.2 to 2 mm in diameter).
3. Analysis of risk factors for recurrence
Logistic regression analysis was used to select risk factors for predicting recurrence. Histological grade/subtype, myometrial invasion (<1/2 vs. ≥1/2), cervical involvement (negative vs. positive), LVSI (negative vs. positive), peritoneal cytology (negative vs. positive), adjuvant therapy (none/radiotherapy vs. chemotherapy), and ultrastaging of LNs (negative vs. ITC or MM) were investigated. For the analysis, two dependent variables were used: (1) recurrence, which means either intrapelvic recurrence or extrapelvic recurrence, and (2) extrapelvic recurrence.
4. Survival analysis
The outcome measures were overall survival (OS) and recurrence-free survival (RFS). OS was defined as the time from commencement of initial treatment to death. RFS was defined as the time from the start of initial treatment to initial recurrence. Patients known to still be alive or lost to follow-up at the time of analysis were censored at their last follow-up. Survival rates were estimated using the Kaplan-Meier method.
5. Statistical analysis
Unpaired numerical data were compared using the Student unpaired t-test. Proportional data were compared using the chi-square test or Fisher exact test. The statistical significance level was set at p˂0.05. Statistical analyses including logistic regression analysis, and Kaplan-Meier methods were performed with StatView J-5.0 (SAS Institute, Cary, NC, USA).
RESULTS
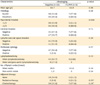
The characteristics of all 61 patients are shown in Table 1. Median follow-up period was 107 months (range, 22 to 190 months). Twenty-six patients (42.6%) had high-risk histology. Thirty-two (52.5%) had deep myometrial invasion. Fifty-two patients (85.2%) underwent pelvic lymphadenectomy without para-aortic lymphadenectomy. Twenty-five (41.0%) did not receive adjuvant chemotherapy. Nine (14.8%) had occult LN metastases, comprising six patients with ITC and three with MM.
Table 1
Clinical characteristics of 61 patients with intermediate-risk endometrial cancer

Relationships between clinical characteristics and ultrastaging results are shown in Table 2. There was a significantly higher rate of deep myometrial invasion in the ITC or MM group than in the node-negative group (88.9% vs. 46.2%, p=0.028), despite there being no significant differences between the two groups in tumor histology, cervical involvement, LVSI, peritoneal cytology, number of LNs assessed, and type of adjuvant therapy.
Table 2
Relationships between clinical characteristics and nodal status confirmed by ultrastaging
Recurrence was observed in 12 patients (19.7%). Recurrence patterns and recurrence sites are shown in Table 3. Intrapelvic recurrence, extrapelvic recurrence, and both intrapelvic and extrapelvic recurrence were observed in five, one, and six patients, respectively. Of the seven patients with extrapelvic recurrence, three (42.9%) experienced para-aortic recurrence.
Table 3
Recurrence pattern and recurrence site in intermediate-risk endometrial cancer

Table 4 shows the results of logistic regression analyses of risk factors relating to recurrence. Although ITC/MM was not a risk factor for recurrence (adjusted relative risk [RR], 3.6; 95% confidence interval [CI], 0.5 to 27.9), it was an independent risk factor for extrapelvic recurrence (adjusted RR, 17.9; 95% CI, 1.4 to 232.2). Implementation of adjuvant chemotherapy was not significantly associated with extrapelvic recurrence (adjusted RR, 0.19; 95% CI, 0.017 to 2.02).
Table 4
Logistic regression analyses of risk factors relating to recurrence and extrapelvic recurrence

Table 5 shows the clinical characteristics of nine patients with ITC or MM. All patients did not undergo para-aortic lymphadenectomy. Two patients (28.6%) did not receive adjuvant chemotherapy. Four patients (44.4%) experienced recurrence. The rate of recurrence was higher in the patients with ITC or MM who did not receive adjuvant chemotherapy than in patients with ITC or MM who did (100% vs. 28.6%, p=0.17). All recurrent tumors occurred in extrapelvic sites, the breakdown of which was as follows: two in para-aortic lymph nodes (PANs), one in PANs/mediastinum, and one in the liver/diaphragm. While no patients without ITC or MM experienced PAN recurrence, 33.3% of patients with ITC or MM experienced PAN recurrence (p=0.002).
Table 5
Clinicopathological findings and outcomes of nine cases with ITC/MM

CI, cervical involvement; CTX, adjuvant chemotherapy therapy; DOD, die of disease ; G1, endometrioid grade 1; G2, endometrioid grade 2; G3, endometrioid grade 3; ITC, isolated tumor cell; LVSI, lympho-vascular space invasion; MI, myometrial invasion; MM, micrometastasis; NED, no evidence of disease ; OS, overall survival; PAN, para-aortic lymph node; PC, peritoneal cytology; RFI, recurrence-free interval; RTX, adjuvant radiation therapy; S, serous adenocarcinoma.
Fig. 1 shows the Kaplan-Meier curves according to ultrastaging nodal status. There was no significant difference in OS (log-rank test, p=0.074) and RFS (log-rank test, p=0.066) between the node-negative and ITC or MM groups. However, the 8-year OS/RFS rates were >20% lower in the ITC or MM group than in the node-negative group (OS, 71.4% vs. 91.9%; RFS, 55.6% vs. 84.0%). Time to recurrence tended to be longer in the ITC or MM group than in the node-negative group (median, 49 months vs. 16.5 months; p=0.080).

DISCUSSION
Patients at intermediate risk of recurrence in whom no LN metastasis is detected by routine microscopic examination may have occult microscopic disease in their LNs. Although previous studies have reported a 3.8% to 19.7% incidence of ultra-stage-detected MM in sentinel LNs of patients with endometrial cancer [1920212223], the subjects of those studies were not necessarily limited to intermediate-risk patients. In the present study, ITC or MM in regional LNs were detected in 14.8% of patients with intermediate-risk endometrial cancer, namely, FIGO stage I to II disease that had at least one of the following recurrent-risk factors: G3 endometrioid/serous/clear cell adenocarcinomas, deep myometrial invasion, cervical involvement, LVSI, and positive peritoneal cytology.
The result of this study raises the question as to why ITC or MM was not a predictor of survival. First, current adjuvant chemotherapy may be effective against ITC or MM that may have been present in the regional LNs. In the present study, implementation of adjuvant chemotherapy reduced the risk of extrapelvic recurrence (RR, 0.19; 95% CI, 0.017 to 2.02), despite this not being significant. While all the patients with ITC or MM who did not receive adjuvant chemotherapy suffered recurrence, only 28.6% of patients with ITC or MM who did suffered recurrence (p=0.17). The authors previously presented the results of the significant survival effect of para-aortic lymphadenectomy (SEPAL) for intermediate- and high-risk patients [7]. According to a result of the SEPAL study, a significant survival benefit of para-aortic lymphadenectomy was not shown in intermediate-risk patients who received adjuvant chemotherapy (hazard risk, 0.68; 95% CI, 0.26 to 1.73) [7]. One plausible explanation for the result is that adjuvant chemotherapy can replace surgical removal as a treatment for LN MM in the para-aortic area. Second, we speculate that ITC or MM may be associated with relatively lower biological aggressiveness. Time to recurrence tended to be longer in the ITC or MM group than in the node-negative group (median, 49 months vs. 16.5 months; p=0.080). It may take quite a long time for tumor deposits of <2.0 mm in the LNs to be presented as clinically detectable recurrent tumors. However, the 8-year OS/RFS rates were >20% lower in the ITC or MM group than in the node-negative group (OS, 71.4% vs. 91.9%; RFS, 55.6% vs. 84.0%) despite being statistically not significant. We cannot exclude the possibility that ITC or MM is a predictor of survival. Unfortunately, there were too few patients in our study to provide conclusive results, and a larger study is required to solve this issue. Although the difference in time-to-recurrence between the ITC or MM and node-negative groups may seem unexpected, such a result can happen. Failure sites are classified into the following groups: lymphatic, hematogenous, peritoneal, and vaginal. While lymphatic recurrences are a typical failure pattern in the ITC or MM group, other types of recurrence may relatively increase in number in the node-negative group. Indeed, in the current study, vaginal recurrences were identified in 50% of patients with relapse in the node-negative group. Isolated vaginal recurrences may be related to early relapse and improved post-recurrence survival.
As a result of our study, we propose one suggestion for the clinical significance of LN MM in endometrial cancer. ITC or MM may be a predictor of extrapelvic recurrence, especially para-aortic node recurrence when implementation of para-aortic lymphadenectomy is not considered. To assess the relationship between surgical resection and recurrence in para-aortic nodes, the present study was conducted with patients who were treated from 1997 to 2004; pelvic lymphadenectomy without para-aortic lymphadenectomy was performed for endometrial cancer patients before 2004 in our institution, but since 2004 it has been our preference to perform para-aortic lymphadenectomy in addition to pelvic lymphadenectomy for patients with endometrial cancer. Therefore, the majority of intermediate-risk patients included in this study did not undergo para-aortic lymphadenectomy. If para-aortic lymphadenectomy is routinely performed, reproducible results regarding relationships between ITC or MM and extrapelvic recurrence may not be obtained.
The result regarding a predictor of ITC or MM also may not be conclusive. While a significant relationship between deep myometrial invasion and ITC or MM were shown in this study, the rate of positive LVSI was twice as high in the ITC or MM group than in the node-negative group, despite not being significant (44.4% vs. 21.2%, p=0.20). LVSI remains a promising predictor of ITC or MM.
The limitations of the present study are as follows. First, the paucity in the number of subjects led to an equivocal conclusion. Second, we handled tumor deposits of <2.0 mm without making distinctions between ITC and MM. In the near future, with the popularization of sentinel node mapping, there will be more data generated for patients with tumor deposits of <2.0 mm. Whether adjuvant chemotherapy at present may be effective or not against ITC or MM in regional LNs is an important clinical question. A multicenter cooperative study is needed to clarify the clinical significance of ITC or MM.
 XML Download
XML Download