

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
According to the World Health Organization classification, there are three categories of endometrial stromal tumors: endometrial stromal nodule, endometrial stromal sarcoma (ESS), and undifferentiated endometrial sarcoma [1]. ESS is the third most common uterine type of sarcoma following leiomyosarcoma and undifferentiated endometrial sarcoma [2]. These tumors, which were previously referred to as low-grade ESS or endolymphatic stromal myosis, have the following distinct characteristics: a young age of onset, high potential for recurrence, indolent clinical course, and hormonal sensitivity with overexpression of estrogen and progesterone receptors. Recurrences develop in 23% to 59% of all patients with ESS [345678910111213141516171819]. According to two recent systematic reviews, 15% to 25% of these patients die of recurrent disease [2021]. All reports of higher mortality rates (19% to 50%) were published more than 30 years ago [478]. In contrast, recent publications have reported that fewer than 10% of patients with ESS eventually die of this disease [1114151718]. High-dose progestins [182223], aromatase inhibitors [2425], and gonadotropin-releasing hormone (GnRH) agonist [2627] are reportedly effective forms of hormonal treatment in patients with advanced or recurrent ESS. Thus, the change in mortality rate of ESS may be attributable to the frequent use of hormonal therapy. In contrast, radiation therapy is relatively ineffective against unresectable ESS [28]. There is also insufficient evidence concerning the efficacy of chemotherapy [29]. The aim of this study was to clarify the clinical outcome of recurrent ESS in the hormone-therapy era.
MATERIALS AND METHODS
1. Patients
This retrospective multicenter study included patients with ESS treated at the following hospitals: Hokkaido Cancer Center, Hokkaido University Hospital, Asahikawa Kosei General Hospital, Sapporo Municipal Hospital, Tomakomai Oji General Hospital, Sapporo Kosei General Hospital, Obihiro Kosei General Hospital, and Hakodate Chuo Hospital. Patients were identified for inclusion through institutional database searches up to 2009. Of the 25 patients with ESS identified by participating institutions, 10 had developed recurrent ESS. Their medical records were reviewed and patient age, the International Federation of Gynecology and Obstetrics stage, relapse-free interval (RFI), relapse site, treatment, response to treatment, duration of follow-up, and clinical outcome extracted.
2. Treatment
Treatments received by eligible patients included surgery, radiotherapy, chemotherapy, and hormonal therapy. All treatments were performed at the discretion of the attending physicians. Hormonal agents used in these patients included medroxyprogesterone acetate (MPA), leuprolide acetate, and dydrogesterone. MPA was administered orally in a daily dose of 400 to 600 mg, leuprolide acetate intramuscularly in a dose of 3.75 mg every 28 days, and dydrogesterone orally in a dose of 15 mg/day. Surgical treatment was classified as complete or incomplete. Response to other treatments was assessed by the Response Evaluation Criteria in Solid Tumors. Thus, complete response (CR) was defined as disappearance of all targets and no evidence of new lesions for at least 4 weeks. Partial response (PR) was defined as at least a 30% decrease in the sum of the longest dimensions of all target measurable lesions, taking as reference the baseline sum of the longest dimensions with no unequivocal progression of non-target lesions and no new lesions. Progressive disease (PD) required at least a 20% increase in the sum of the longest dimensions of target lesions or the appearance of new lesions or death due to disease. Stable disease (SD) was any condition not meeting the above criteria. Response to chemotherapy or hormonal therapy following complete surgery was regarded as not evaluable (NE). Where chemotherapy and hormonal therapy or radiotherapy and hormonal therapy had been used concurrently, the response to each individual therapy was also regarded as NE. The response rate was defined as the sum of CR and PR occupied on all evaluable occasions (CR+PR/CR+PR+SD+PD). Disease control rate was defined as the sum of CR, PR, and SD occupied on all evaluable occasions (CR+PR+SD/CR+PR+SD+PD).
3. Survival analysis
The survival outcome measures used were RFI and post-relapse survival (PRS). RFI was defined as the time from initial treatment of primary tumor to first evidence of relapse. PRS was defined as the time from first evidence of relapse to death from any cause. Living patients were censored at the date of last follow-up.
RESULTS
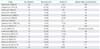
Table 1 shows the clinical characteristics of the 10 study patients. Their median age at the time of initial relapse was 51.5 years (range, 43 to 69 years). All patients were diagnosed as having stage I disease at the time of initial treatment and all underwent surgery including hysterectomy. Eight patients did not undergo bilateral salpingo-oophorectomy at the time of initial surgery. Although complete resection was achieved in all patients, two patients received adjuvant chemotherapy and three adjuvant hormonal therapies. The most frequent site of initial relapse was the ovary (60.0%), followed by the pelvis (40%). Lymph node recurrence occurred in two patients (20.0%). Six of the eight patients (75.0%) who had not undergone surgical castration had ovarian relapses.
Table 2 shows the clinical outcome of the 10 study patients. The median duration of follow-up from initial treatment of primary tumor was 223.5 months (range, 72 to 349 months). Eight patients (80.0%) were alive at the last time of their follow-up. Two patients had died, one at 72 and the other at 280 months. The median RFI prior to initial relapse was 66.5 months (range, 28 to 159 months). The 10-year PRS rate was 90.0% and the median PRS 119 months (range, 7 to 216 months). Fig. 1 shows the RFI curve and the PRS curve for patients with recurrent ESS.
Information regarding initial relapse is shown in Table 3. As to treatments for initial relapse, surgery was performed in nine cases and heavy ion radiotherapy in one. Complete resection of tumors was achieved in four of the nine patients who underwent surgery (44.4%). However, complete remission was finally achieved in eight cases (80.0%).
Information regarding second/subsequent relapses is shown in Table 4. Of the eight patients with complete remissions after treatments for initial relapse, four (50.0%) had second relapses, which took the form of intra-abdominal recurrence in all of them. As to treatments for second relapse, surgery was performed in three cases and hormonal therapy alone in one. Complete resection of tumors was achieved in two of the three patients who underwent surgery (66.7%). Complete remission was finally achieved in two cases (50.0%) after treatment for second relapse. Both patients with complete remissions had a third relapse; one developed tumor embolism in the inferior vena cava and the other multiple lung metastases. One of these patients underwent repeated complete surgical resections on each occasion of subsequent relapse.
Complete resection was achieved on 9/16 occasions (56.0%) when surgery was performed for recurrent disease (Supplementary Table 1). There was no statistically significant difference between initial recurrent tumors and second/subsequent recurrent tumors in the rate of complete resection (44.4% vs. 71.4%, respectively; p=0.36). Of the 11 evaluable occasions of hormone therapy for recurrent disease, the agent used was MPA in eight instances, leuprolide acetate in two, and dydrogesterone in one. The median duration of hormonal therapy was 17 months (range, 2 to 121 months). The response rate was 63.6% and disease control rate 72.7%. One patient had SD for the 68 months, during which she received 600 mg/day MPA as treatment for a third relapse. There was no difference in disease control rate between initial recurrent tumors and second/subsequent recurrent tumors (85.7% vs. 50.0%, respectively; p=0.49). A higher response rate was achieved with initial recurrent tumors than with second/subsequent recurrent tumors (85.7% vs. 25.0%, respectively; p=0.08).
DISCUSSION
The post-recurrence clinical course of ESS has not so far been well described because a long period of time is needed to assess it. The median durations of follow-up in earlier reports ranged from 46 to 130 months [345678910111213141516171819]. In contrast, our median follow-up of 223.5 months (range, 72 to 349 months) is markedly longer than those of previously published studies. The followings are the three major findings of our study. First, the median PRS of our patients with recurrent ESS was >10 years. It was actually 119 months; however, it must be 10 years or more because only 20% of eligible patients had died by the time of final analysis. Second, hormonal therapy was extremely effective against initial recurrent tumors, achieving CRs in four of the five patients (80.0%) with unresectable initial recurrent tumors. Third, hormonal therapy was also clinically effective against second/subsequent recurrent tumors. Two-thirds of the patients with second recurrent tumors who received MPA achieved PRs. ESS has been described as an indolent tumor with a tendency to late recurrence. Our data show that recurrent ESS also behaves indolently. Mortality rates in ESS seem to have decreased during the last three decades (Table 5) [345678910111213141516171819]. The frequent use of hormonal therapy may be largely responsible for this change in mortality rate.
One of the issues we have identified is of some concern. Although hormonal agents are extremely effective against initial recurrent tumors, we observed no CRs to these agents in patients with second/subsequent recurrences and no complete or PR in those with third/subsequent recurrences. These findings suggest that hormonal agents are more effective against initial recurrent tumors than against second/subsequent recurrences.
Because ESS is characteristically indolent and hormonal therapy is remarkably effective, long-term administration of hormonal agents is a topic that requires further investigation. It is well known that the adverse effects of high-dose progestin therapy include thromboembolic complications, weight gain, and depression [30]. Although high-dose progestin therapy has been considered to be well tolerated, in earlier studies oral MPA was only administered for short periods for treatment of advanced or recurrent endometrial cancer [31]. Mizuno et al. [18] evaluated the effects of long-term, high-dose MPA with an anti-platelet agent (aspirin, 100 mg/day) and observed no thromboembolic complications over a median duration of 63 months (range, 28 to 92 months). Use of an anti-platelet agent may prevent thromboembolic events during high-dose MPA therapy. The adverse effects of GnRH agonists are caused by a lack of estrogen, long-term use of GnRH agonists causes osteoporosis [3233]. Adverse effects of aromatase inhibitors are also associated with a deficiency of estrogen; these include musculoskeletal stiffness and pain, fatigue, hot flushes, and nausea [2434]. There is reportedly a high rate of non-compliance with letrozole therapy in breast cancer patients, the overall probability of non-compliance being 18.4% over this study's 2.5 years of follow-up [34]. The most frequent adverse events are musculoskeletal-related symptoms [34]. Dydrogesterone is a hormonally active, non-androgenic synthetic steroid that was developed in the 1950s [35]. Its molecular structure is almost identical to that of natural progesterone, which accounts for the lack of estrogenic, androgenic glucocorticoid, and mineralocorticoid properties [36]. Therefore, dydrogesterone is preferable to other progestins such as MPA because of the lack of adverse effects of long-term medication or repeated courses of treatment [36]. One patient in the present study (Case 4) experienced troublesome adverse effects of a GnRH agonist; subsequent use of dydrogesterone was effective [37].
Hysterectomy with bilateral salpingo-oophorectomy is generally considered a standard surgical treatment. However, it has been shown that ovary-sparing surgery does not worsen survival outcome [10111214163839]. In the present study, the median overall survival time of the eight patients who did not undergo surgical castration at the time of initial surgery was 230 months (range, 72 to 349 months), despite six of these patients (75.0%) subsequently developing ovarian recurrences. The present findings encourage us to perform ovarian-sparing surgeries, especially in women with ESS of reproductive age. On the other hand, in large population-based studies lymph node metastases have been noted in less than 10% of patients undergoing lymphadenectomy [3839]. While the prognostic significance of lymph node involvement is controversial, lymphadenectomy does not improve the prognosis of ESS [143839]. In this study, lymph nodes were one of the initial failure sites in two patients. Although these patients were found to have nodal recurrences relatively soon after their initial surgery, both remain alive with PRS times of 82 and 184 months. Thus, our findings do not support routine lymphadenectomy at the time of initial treatment.
In this retrospective study, there were too few patients to draw any definitive conclusions. However, it will always be difficult to conduct a prospective study aimed at assessing the long-term clinical course of recurrent ESS because of the rarity of ESS and its indolent clinical course. PRS of patients with recurrent ESS can be expected to be >10 years when treated by repeated surgical resection and hormonal therapy or both.





 XML Download
XML Download