

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
The aim of this paper was to describe the operative details for en bloc removal of the adnexal tumor, uterus, pelvic peritoneum, and rectosigmoid colon with colorectal anastomosis in advanced epithelial ovarian cancer patients with widespread pelvic involvement.
Methods
The patient presented with good performance status and huge pelvic tumor extensively infiltrating into adjacent pelvic organs and obliterating the cul-de-sac. The patient underwent en bloc pelvic resection as primary cytoreductive surgery. En bloc pelvic resection procedure is initiated by carrying a circumscribing peritoneal incision to include all pan-pelvic disease within this incision. After retroperitoneal pelvic dissection, the round ligaments and infundibulopelvic ligaments are divided. The ureters are dissected and mobilized from the peritoneum. After dissecting off the anterior pelvic peritoneum overlying the bladder with its tumor nodules, the bladder is mobilized caudally and the vesicovaginal space is developed. The uterine vessels are divided at the level of the ureters, and the paracervical tissues (or parametria) are divided. The proximal sigmoid colon is divided above the most proximal extent of gross tumor using a ligating and dividing stapling device. The sigmoid mesentery is ligated and divided including the superior rectal vessels. The pararectal and retrorectal spaces are further developed and dissected down to the level of the pelvic floor. The posterior dissection is progressed and moves to the right and then to the left of the rectum. The rectal pillars including the middle rectal vessels are ligated and divided. Hysterectomy is completed in a retrograde fashion. The distal rectum is divided using a linear stapler. The specimen is removed en bloc with the uterus, adnexa, pelvic peritoneum, rectosigmoid colon, and tumor masses leaving a macroscopically tumor-free pelvis. Colorectal anastomosis was completed using stapling device.
Results
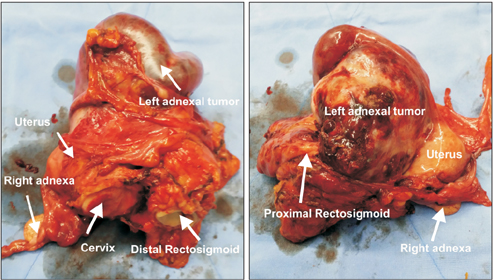
En bloc pelvic resection was performed by total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic peritonectomy, and rectosigmoid colectomy with colorectal anastomosis using a stapling device. Complete clearance of pelvic disease leaving no gross residual disease was possible using en bloc pelvic resection.
 XML Download
XML Download