

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
We have used transabdominal ultrasound (TAUS) for the placement of the intrauterine tandem in cervix cancer patients during brachytherapy since 1985. Magnetic resonance imaging (MRI) was introduced in our practice to image pretreatment cervix tumor in 1996. Initially it was used for measuring the tumor volume and assessing the position of the uterus within the pelvis to determine external beam radiotherapy (EBRT) field borders [1]. Following acquisition of an high dose rate (HDR) after loader and MRI compatible tandem and ovoids (T&O), MRI was used to optimise the dose to bladder and rectal points as specified by International Commission on Radiation Units and Measurements (ICRU) report No. 38 while prescribing the dose to point A [2]. Gradually it became apparent that the ultrasound image taken during the placement of tandem could be compared with MRI of the applicator in the treatment position and confining isodose to the cervix and uterus. The ultrasound based plan was back projected onto the MRI and adapted for subsequent insertions if necessary. Use of ultrasound at each following insertion meant that plans could be verified and modified if needed. Use of low dose rate (LDR) brachytherapy for cervix cancer gradually declined after the introduction of the high dose rate (HDR) unit in 1998. By 2001 all patients were treated with HDR brachytherapy. Our initial experience with HDR conformal brachytherapy for cervix cancer using TAUS and comparative results between LDR and HDR conformal brachytherapy has been published [3].
The aim of this study was to report on the long-term results of ultrasound guided conformal brachytherapy in cervix cancer patients with respect to patterns of failures, treatment related toxicities, and survival.
MATERIALS AND METHODS
1. Patient selection criteria
Three hundred and nine newly diagnosed cervix cancer patients, who were previously untreated and presented to The Peter MacCallum Cancer Centre, between January 1999 and December 2008 were retrieved from a prospective gynaecology service database. All patients were treated with EBRT using a four field box technique and high dose rate image guided conformal brachytherapy (HDRc) with curative intent. Of these, three patients with serous histology, ten with small cell histology, one with malignant mixed Müllerian tumor, and three patients with International Federation of Gynecology and Obstetrics (FIGO) stage IV disease were excluded from the analysis. All patients were clinically staged using FIGO staging criteria. In addition, 253 patients were staged using both MRI and positron emission tomography (PET), 18 had MRI and no PET, 18 had PET and no MRI, and three patients refused pretreatment MRI and PET scan. MRI and PET information was not used to change clinical FIGO staging as reported in this paper.
2. Treatment
Radiotherapy (RT) of cervix cancer as used in this study has been previously described [4]. All patients received weekly cisplatin 40 mg/m2 during the course of their EBRT (unless contraindicated).
All patients were treated using four fields. Node negative patients were treated with pelvic fields, the upper border of which was located at L5 to S1. Patients with metastatic nodes confined to the pelvis were also treated with pelvic RT in prone position on a belly board. The patients with common iliac or para-aortic nodes (n=48) were treated supine with 4-field extended field radiotherapy (EFRT). The upper border of the para-aortic field was kept 4 cm above the upper most involved node. EFRT usually extended between the lower border of L3 to the upper border of L1. Involved nodes received a rectangular boosts of 6 to 10 Gy in 2 Gy fractions. Nodal boosts, when needed were given between intracavitary brachytherapy. No parametrial boosts were given. Patients treated with pelvic field RT received 40 Gy in 2 Gy fractions and those with EFRT received 45 Gy in 1.8 Gy fractions.
3. HDR image guided conformal brachytherapy
HDRc was always given at the completion of EBRT. Initial dose and fractionation was six fractions of 5.2 Gy (equivalent dose 2 [EQD2], 39.5 Gy; n=14), prescribed to point A with dose optimisation to ICRU bladder and rectal points. From 2000 to 2002 HDRc was changed to a dose of 30 Gy in 5 fractions (EQD2, 40 Gy; n=119), or 28 Gy in 4 fractions (EQD2, 39.7 Gy; n=112) given twice weekly. In a few patients (n=37) HDRc consisted of 3 factions of 8.5 Gy (EQD2, 39.3 Gy) each [5]. This was due to unavailability of the treatment unit over public holidays and was necessary to maintain overall treatment time within 8 weeks. Dose was prescribed to a target as determined by TAUS and confirmed by MRI.
The procedure for T&O placement and brachytherapy target delineation, target outline measurements using ultrasound and recording of the measurement on graph paper have been previously described (Fig. 1) [6].
Briefly, the brachytherapy dose was prescribed to the perimeter of the target. The target consisted of residual tumor containing cervix and the body of uterus in the sagittal plane. A thin rind of fundal tissue was usually spared, as infiltrating cervical tumor almost never extended to the uterine fundus. This also ensured sparing of bowel loops that were frequently seen around the uterus, especially near the fundus. No special efforts were made to identify the pretreatment extent of tumor in the vagina or parametrial extension. Intent was to treat residual disease, cervix and uterus (as defined by ultrasound) to a total dose of 80 Gy10 to 96 Gy3 expressed in 2 Gy EQD2. Total doses and individual HDRc fractions were calculated using a table described by Nag and Gupta [7]. The first fraction was planned using the corpus and cervix dimensions measured on ultrasound in sagittal and axial plane [3]. There was no patient movement between ultrasound based planning and the first treatment as patient remained under anaesthesia. Following treatment, the patient was sent to the MRI suite for a planning MRI with applicators in treatment position. Differences in the measurements of the cervix and uterus obtained by MRI and ultrasound were within clinically acceptable limits [8]. Following the MRI, the applicator was removed and the patient was sent home. Once standardised, time taken to image, plan, and treat a new patient took was about 90 minutes following spinal anesthesia. Subsequent insertions and treatments were performed under general anaesthesia and usually took 60 to 90 minutes. TAUS was always used to reproduce the position of the tandem within the uterus, and the position of the uterus in the pelvis in relation to the sacrum and in relation to the catheter balloon in the bladder. The radiation dose (EQD2, 39.3 to 40 Gy) was prescribed at the target surface and incident point A doses, ICRU 38 bladder and rectal point doses were recorded in 2 Gy EQDs (by adding EBRT doses and EQD2 brachytherapy doses). Follow-up and criteria for assessing outcomes has been previously described [5]. All follow-up data was prospectively collected at the time of patient's routine appointments. Toxicities were scored according to modified WHO/RTOG criteria. Three categories of toxicities to organs at risk consisting of bladder, small and large bowel, and vagina have been included in this study.
4. Statistical analysis
A close-out date for this study was defined as the earliest of the last appointment date or follow-up date for patients who are alive and not lost to follow-up. All events after this date were censored to minimise any potential bias. Overall survival (OS) was defined as the time difference between the date of diagnosis to date of death irrespective of the cause of death. Failure free survival (FFS) was defined as the time difference between date of diagnosis and date of first failure or death. Kaplan-Meier curves for OS and FFS were calculated from which 5-year event-free rates were determined. Prognostic factors were evaluated using both uni and multivariate Cox proportional hazards model. Prognostic factors evaluated include age, FIGO stage, histology, tumor volume, parametrial invasion, and nodal status. The impact of prognostic factors on OS and FFS were summarised using hazard ratios (HR) along with 95% confidence intervals (CIs). Apart from FFS (defined as failure at any site), prognostic factors were evaluated for each of the following specific sites: primary and pelvic, para-aortic and distant sites. Descriptive statistics were used to present toxicities associated with treatment.
RESULTS
Two hundred and ninety-two patients were available for analyses. The median (interquantile range [IQR]) follow-up time was 4.1 years (2.4 to 6.1 years). All observations were censored on the 15th January 2011. Two patients were lost to follow-up at 73 and 620 days following the commencement of their RT. Patient characteristics are described in Table 1.
Median tumor volume was 37.5 cm3, 66.8% patients had tumor invasion in to the corpus and 45% patients had positive nodes. EFRT was used in 16.4% patients and the rest of the patients received pelvic RT.
1. Failure free survival and overall survival
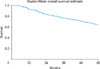
At the cut-off date when 98 patients had relapsed, 24 were alive with disease, and 103 patients had died. Of these, 29 died without any failure and two patients were lost to follow-up. One hundred and sixty-five were alive without any relapse. Five year FFS and OS were 66% (95% CI, 60 to 71) and 65% (95% CI, 58 to 70), respectively. OS is shown in Fig. 2.
Univariate analysis of FFS and OS at 5 years was studied. Several prognostic factors including age, FIGO stage, histology, tumor volume, parametrial invasion on MRI and fluorodeoxyglucose avid nodes were analysed. Association of prognostic factors for FFS and OS are shown in Table 2. On multivariate analyses, tumor volume, and node positivity were independent predictors for both FFS and OS (not shown).
2. Sites of failure
Ninety-eight patients experienced relapse at 5 years. Most of the patients in the present study had a posttreatment PET at 4 to 9 months after treatment. This was repeated if there was any clinical suspicion of recurrence. Overall, primary site (cervix and uterus), pelvic, para-aortic failure, and distant failure were observed in 12.5%, 16.4%, 22%, and 23%, respectively. Local relapses according to FIGO stage I, II, and III were 12%, 10%, and 17%, respectively. Of those who had a recurrence at primary site, median time to recurrence was 9.2 months (IQR, 3 to 52 months). Those who failed at the primary sites were five times more likely to fail simultaneously at the para-aortic site and 4.3 times more likely to fail at distant sites. This relationship was independent of primary site failure. Eighty patients (82%) failed within 2 years and the rest after 2 years. Median survival of patients relapsing within 2 years and after 2 years was 23.7 and 56.6 months, respectively.
Two hundred and forty-four patients were treated with pelvic RT, of these 71 patients (29%) failed. Ten relapsed exclusively within irradiated field. These include two primary site failures only and both were salvaged by hysterectomy. Eight patients relapsed only in para-aortic nodes, of these seven were salvaged either by chemoradiotherapy or surgery and chemoradiotherapy. The remaining 53 patients relapsed at multiple sites including 47 patients who relapsed beyond para-aortic nodes and distant sites.
Forty-eight patients received EFRT, of these 27 (56%) have relapsed. Of these, three failed exclusively in the treated volume and, 17 failed both inside and outside the treated volume. These contained seven patients who had only failed outside the treated volume. Of the three patients who failed in the treatment volume, two failed at multiple sites and one failed only at the margin of para-aortic node (a marginal relapse). This patient was successfully salvaged by repeat chemoradiotherapy. Thus only 7/292 patients died exclusively of disease recurrence in the treatment field.
3. Effects of prognostic factors on the site of failure
In multivariate analyses, tumor volume was significantly associated with primary site failure (HR, 1.7) and pelvic failure (HR, 2.1). For para-aortic failure, corpus involvement (HR, 2.0) and positive nodes (HR, 2.4) were independently significant. Distant failure was associated with tumor volume (HR, 1.6) and positive nodes (HR, 7.8).
The mean tumor dose was 80.1 Gy (range, 52.3 to 100.0 Gy; SD, 5.5) and point A dose was 69.4 Gy (range, 40.5 to 101.1 Gy; SD, 9.7). In conformal brachytherapy, the dose prescription was unrelated to point A. Since brachytherapy plays an important role in the local control of cervix cancer the interaction between local failure, tumor dose (target dose) and point A dose was further explored. The dose to point A was inversely related to local control (p=0.017). This inverse prognostic significance of dose to point A was retained even after adjusting for node positivity and tumor volume. When point A dose was analysed in quartiles, the highest quartile group had the highest primary failure rates (p=0.022; HR, 3.6).
4. Factors affecting point A, ICRU bladder and rectal point doses and late toxicities
Median (IQR) target, point A, ICRU38 bladder and rectal doses were 80 Gy (IQR, 79.7 to 80.4 Gy), 68.2 Gy (IQR, 62.5 to 77.2 Gy), 53.4 Gy (IQR, 48 to 63 Gy), and 55.5 Gy (IQR, 51.3 to 62 Gy) respectively. Each increment increase in point A dose increased the risk of primary failure by 4.6% (p=0.008).
Dose at point A was independent of pretreatment tumor volume. There were 147 patients at or above median point A dose level. In these patients the pretreatment mean tumor volume was 33.84 cm3. In the remaining 145 patients the mean tumor volume was 43.9 cm3 (p=0.045). The highest recorded toxicities per site are shown in Table 3.
There was no correlation between the median doses to various ICRU38 dose points and the observed toxicities. Grade 3 and 4 bladder toxicity had a rate of 0.3 per 100 person years of follow-up. Grade 3 and 4 bowel toxicity had a rate of 0.99 per 100 person years of follow-up. Grade 3 and 4 vaginal toxicity had a rate of 0.69 per 100 person years of follow-up.
DISCUSSION
It is generally agreed that local control of the primary cancer is associated with a higher survival in cancer patients. In those patients where primary treatment is RT, a pertinent question to ask would be "if we could eliminate local-regional failures and treatment related morbidity, what would be the gain in survival?" [9]. With the application of precision RT [10,11,12], it has now become possible to achieve adequate locoregional control while limiting the treatment related side effects. In addition to FIGO staging (n=292), 271 patients (93%) had their pretreatment tumor volume measured with MRI and the same number of patients had nodal status known through PET. Thus, the precise extent of the disease was known and included within the treatment volume minimising the risk of failure due to untreated disease. The follow-up data was collected prospectively and all sites of initial and subsequent site of relapses were recorded using posttreatment PET and or clinical and radiological evidence of disease progression.
In conformal brachytherapy as described in this study, the dose was prescribed to the residual tumor volume at the end of EBRT hence the incident dose to point A varied widely. Patients with exophytic disease and corpus noninvasive tumors usually do not have positive nodes [13]. These tumors also register a good response to EBRT. Thus at the time of brachytherapy the residual tumor volume is small and when the brachytherapy dose is prescribed to the residual tumor, the prescription line usually falls medial to point A, registering lower point A doses. These patients being node negative also have a better prognosis. Conversely, infiltrative, corpus invasive and node positive tumors respond poorly to EBRT and may still retain a larger diameter such that the target surface may lie on isodoses passing through or lateral to point A, registering a higher point A dose. Infiltrative and node positive patients have poor prognosis [14]. Hence the paradox of conformal brachytherapy, where lower point A dose group has better prognosis as compared to the group receiving higher point A dose.
Five year local control was achieved in 87.5% of patients. Median time to recurrence at the primary site was 9.2 months (IQR, 3 to 52 months). Local control was comparable to 89% at 2 years, 95% at 3 years, and 91% at 3 years as reported by Haie-Meder et al. [15], Potter et al. [16], and Lindegaard et al. [17] respectively. All had used MRI based conformal brachytherapy using GEC-ESTRO recommendation [18]. Most of the patients in the present study had a post treatment PET at 4 to 9 months after treatment. This was repeated if there was any clinical suspicion of recurrence. Thus it was possible to detect any asymptomatic recurrences earlier. There were some differences between the current study and other reported studies. In the study by Haie-Meder et al. [15], 49/84 patients underwent total hysterectomy at the completion of chemoradiotherapy. No patients in the present study underwent completion hysterectomy. Potter et al. [16] used combined interstitial needles with intracavitary applicators in 44% of their patients. Patients in our study were mainly treated using T&O applicators with occasional use of a tandem and cylinder combination in those patients with stage 3A disease or in patients with a very narrow vaginal vault. None had received interstitial brachytherapy. Lindegaard et al. [17] used a mean dose of 91 Gy (EQD2) for the high risk clinical target volume. The primary tumors in Lindegaard's study were treated more aggressively compared to the present study where the median dose to target was 80 Gy (EQD2). Our brachytherapy target consisted of residual tumor, cervix and uterine body. At the fundus, a 5 to 10 mm of uterine rind was spared as described earlier [19]. We had neither used parametrial boost (in node negative patients) nor have we looked for or tried to cover the so-called grey zone or intermediate-risk tumor volume [20]. According to a study by Schmid et al. [21], grey zones appear to represent a substantial proportion of the residual tumor volume at the time of brachytherapy although the tumor viability post EBRT in this region could not be ascertained.
In the present study the local failure rate among the node negative and node positive patients was 9% and 16% respectively. Although the node positivity was not statistically significant for local failure, it was significant for nodal and distant failure (HR, 3.70) [14] and was unrelated to the control of the primary site. Addition of interstitial needles [16] and hysterectomy [15] to conformal intracavitary brachytherapy delivering well in excess of 85 Gy (EQD2) to augment local control, resulted in OS at 3 and 4 years of 68% and 57%, respectively; no better than 5 years OS of 66% in the present series. Out of 71 patients who relapsed, only 13 patients recurred in the irradiated volume. All other failures were multisite failures. It is unlikely that failure outside treated volume in PET and surgically staged patients could be due to pre-existing undiagnosed microscopic metastatic disease. Such excess of relapses were also observed by Delpech et al. [22] in patients with FIGO stage IB2 and II, who had full course of curative chemoradiotherapy followed by hysterectomy and lymphadenectomy. Delpech et al. [22] were surprised to find more than twice the incidence of para-aortic nodal involvement (18%) following a full course of chemoradiotherapy, in comparison to 8% patients with positive para-aortic nodes in similar stages whom they had treated earlier with primary surgery [23]. More aggressive therapy at the primary site has been shown to be associated with increased morbidity without any improvement in OS [24].
We had meticulously encouraged patients (at every follow-up appointment) to use vaginal cylinder and oestrogen cream following RT. Our maximum mucosal dose (measured at the lateral surface of the ovoids was usually kept at 120 Gy3 (EQD2). Similarly, the ICRU38 bladder and rectal doses were 53.4 and 55.5 Gy, respectively. It is surprising that late effects in our patients were comparable to those published in other series using higher doses to the target, parametria, and vaginal surface.
In conclusion, using ultrasound guided conformal brachytherapy for cervix cancer we have been able to achieve optimal local control and OS. The Melbourne protocol compares favorably to more technically elaborate and expensive GEC-ESTRO based protocols. The technical simplicity of using real-time imaging and treatment planning makes this method the method of choice for treatment of cervix cancer in most parts of the world where cervix cancer remains a major health problem and MRI is inaccessible [25].




 XML Download
XML Download