

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ovarian carcinoma is the leading cause of death in all the gynecologic cancers in most developed countries, despite recent improvement of treatment modalities [1,2]. There have been many reports investigating prognostic factors for the ovarian cancers such as International Federation of Gynecology and Obstetrics (FIGO) stage, residual tumor diameter, response of the first-line chemotherapy [3-5]. After maximal cytoreductive surgery, however, all the patients receive combination therapy with paclitaxel and carboplatin regardless of histological subtypes [6,7].
Clear cell carcinoma (CCC) of the ovary is a distinctive histological subtype characterized by clear cells growing in solid/tubular or glandular patterns as well as hobnail cells [8]. The proportion of clear cell carcinoma is relatively low in non-Japanese population, ranging from 3.7% to 12.1% [9-12]. However, in Japan, CCC accounted for 24.2% of all epithelial ovarian cancers, and the proportion has been increasing [13]. A report demonstrated the age-standardized rate (ASR) of CCC was significantly increased in not only older ages (>50), but also in younger ages (<50) [14].
Recent studies confirmed the evidence that CCC showed resistant phenotype against many chemotherapeutic agents [15-20]. There have been still arguments over prognoses of SAC and CCC disease [21,22]. These reports compared the prognosis according to FIGO stage distribution only, and did not include the variables of residual tumor diameter and peritoneal cytology status. The aim of the present study is to compare prognoses of the patients with CCC and serous adenocarcinoma (SAC) and to investigate the impact of CCC histology using multivariable analysis.
MATERIALS AND METHODS
1. Patients and tumors
Among patients with epithelial ovarian cancers treated between January 1984 and September 2009, cases with CCC and SAC were enrolled in the present study. Histological subtypes were confirmed by central pathologic review by two independent pathologists, and medical charts of the patients were analyzed retrospectively. Tumors were diagnosed as CCC if typical clear or hobnail cells growing in a papillary, solid, or tubulocystic pattern are presented in >90% of all pathologic specimens. Mixed type was excluded from the present study. Of all the patients treated in those hospitals, the following patients were selected: 1) patients who underwent primary debulking surgery; 2) patients whose tumor specimens were confirmed as CCC or SAC; 3) patients whose medical charts were assessable. The patients that received neoadjuvant chemotherapy as primary therapy were excluded from the study.
Staging was performed according to FIGO system, and optimal surgery was defined as the cytoreductive surgery achieving residual tumor less than 1 cm in diameter. For the analysis of stage I patients, complete surgical staging procedure was determined: completion of all procedures including hysterectomy, bilateral salpingo-oophorectomy, peritoneal washing, omentectomy, pelvic lymphadenectomy and para-aortic lymphadenectomy. Pelvic lymphadenectomy needed removal of all pelvic nodes from the common, external and internal iliac node, obturator vessel, and the inguinal node. For the completion of para-aortic lymphadenectomy, dissection of all nodes located from the bottom of the left renal vessel until bifurcation of the aorta was needed. The cases that underwent only biopsy of pelvic or para-aortic lymph nodes were not included in complete surgical staging procedure. The resected lymph node counts were not considered for the completion of the lymphadenectomy. In the present study, stage I disease was considered as 'early-stage' disease, and stage II-IV disease was defined as 'advanced-stage' disease.
Primary chemotherapy was classified into three categories: conventional platinum-based, taxane+platinum, and irinotecan+platinum therapy. Conventional platinum-based chemotherapy included cyclophosphamide and platinum (CP) or cyclophosphamide, doxorubicin, and platinum (CAP) or epirubicin and platinum (EP). Taxanes and platinum (taxane-platinum) was comprised of paclitaxel/docetaxel plus carboplatin, and irinotecan+platinum included irinotecan plus cisplatin/carboplatin.
Response rate was evaluated by using Response Evaluation Criteria in Solid Tumors (RECIST) criteria. The images of computed tomography or magnetic resonance were evaluated every two cycles of chemotherapy. Serum levels of tumor markers including CA-125 were not used for progression in the present study. The time to progression was defined as the interval from the date of primary surgery until the date of progressive disease (PD). Survival duration was determined as the time from the date of primary surgery or the date of initial neoadjuvant chemotherapy until death or the date of last follow-up contact. The study protocol was approved by the Institutional Review Board of National Defense Medical College.
2. Statistical analysis
Kaplan-Meier method was used for calculation of patient survival distribution. The significance of the survival distribution in each group was tested by the log-rank test. The chi-square test and Student's t-test for unpaired data were used for statistical analysis. Cox proportional hazards model was used for multivariate analysis of the survival. The variables for multivariate analysis in patients with stage I were age (<60 vs. ≥60), surgery (complete vs. incomplete), histological subtype (CCC vs. SAC). The variables for the stage II/III/IV cases were age (<60 vs. ≥60), stage (III/IV vs. II), histological subtype (CCC vs. SAC), residual tumors after the primary surgery (0 cm vs. present), and chemotherapy (conventional platinum-based vs. others). A p-value of <0.05 was considered statistically significant. The StatView ver. 5.0 (SAS Institution Inc., Cary, NC, USA) was used for statistical analysis.
RESULTS
Between January 1984 and September 2009, a total of 500 patients with ovarian cancers were treated at our hospital. Among them, 111 (22%) patients with CCC and 199 (40%) patients with SAC were identified, and enrolled in the present analysis. The median follow-up period of the patients with CCC and SAC was 71 months and 56 months, respectively.
Patient's characteristics were shown in Table 1. Median age was 55 years in SAC and 52 years in CCC, suggesting younger patient population for CCC (p=0.030). Number of stage I patients was significantly higher in CCC than that of SAC disease (55% vs. 13%, p<0.001). The cases who achieved no residual surgery were 79 (71%) patients in CCC, and 92 (46%) patients in SAC tumors (p=0.0001). Imbalance of primary chemotherapy was also observed: more SAC cases in taxane+platinum regimen, and more CCC cases in irinotecan+platinum therapy (p<0.001). Significantly higher response rate was documented in SAC disease in comparison with CCC tumors (73% vs. 25%, p<0.001). All physicians in our institution recommended postoperative chemotherapy for all patients with CCC. Despite our suggestion, some patients rejected the further therapy. Therefore there were some cases that did not receive primary chemotherapy: 11 cases in CCC, and 25 patients in SAC. All cases with no primary chemotherapy had stage I tumor only.
Five-year progression-free survival (PFS) and overall survival (OS) was shown in Table 2. According to FIGO stages, there were no significant differences of PFS and OS in stage I, II, and IV patients between CCC and SAC group. However, PFS and OS of stage III CCC patients were significantly shorter than those of SAC tumors.
Subsequently, 60 patients with stage I CCC and 27 patients with stage I SAC were further analyzed by multivariate analysis. Positive peritoneal cytology was identified as an independent poor prognostic factor for PFS (hazard ratio [HR], 2.82; p=0.04) and OS (HR, 3.57; p=0.049) (Table 3). In addition to age and extent of surgical staging procedure, histology was not a prognostic factor in stage I disease.
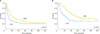
The patients with stages II-IV disease were further evaluated using multiple regression analyses: 51 patients with CCC and 172 patients with SAC (Table 4). Other than factors of age and chemotherapy, three factors were identified as prognostic factors for both PFS and OS. CCC histology was an independent factor for PFS (HR, 2.44; p<0.01), and OS (HR, 2.59; p<0.01). Survival curves of the patients with stage II-IV tumors clearly demonstrated that PFS and OS were significantly shorter in CCC compared with those in SAC patients (Fig. 1).
DISCUSSION
According to recent reports comparing survival of CCC patients with that of SAC cases, there have been no significant difference of OS between those two histologic subtypes among stage I carcinomas of ovary demonstrated [9,11,15]. On the other hand, a study based on Surveillance, Epidemiology and End Results (SEER) database suggested that the patients with stage I CCC had poorer OS than patients with SAC [4]. However, other clinicopathologic factors such as peritoneal cytology, chemotherapy, and extent of surgical staging were not available in the data from SEER, although the independent poor prognostic factors of pT1M0 CCC were positive peritoneal cytology [23]. A subset analysis of a prospective phase III trial enrolling early-stage ovarian cancers revealed that there were no significant difference of PFS and OS between CCC and SAC [21]. Of note, Sugiyama et al. [15] suggested that OS of stage IC CCC was worse than that of stage IC SAC, although p-value did not reach a statistical significance. On the other hand, a consensus report from the first ovarian clear cell symposium suggested that early-stage CCC had a better outcome than that of high grade SAC of same stage; however, the results were not based on multivariate analyses [22]. The present study demonstrated that CCC histology was not a prognostic factor in stage I disease, and that peritoneal cytology was the only significant factor for PFS and OS. The results suggested by Sugiyama et al. [15] were in agreement of the present study, in that the status of peritoneal cytology was important for early-stage CCC ovarian cancers [23,24]. For the analysis of early-stage ovarian tumors, clinicopathologic factors including peritoneal cytology seem to be inevitable, as CCC showed chemo-resistant phenotype.
Our study identified CCC as one of the independent prognostic variables for PFS and OS of stage II-IV disease. So far, there also have been arguments in survival of advanced cases between CCC and SAC. Several studies showed significant worse survival in advanced CCC [4,15,22], however, others did not find difference of OS between CCC and SAC [16,25]. The difference might be derived from other factors such as residual tumor, or pathological heterogeneity. The present study excluded mixed epithelial ovarian cancers, as previous report suggested that patients with mixed epithelial cancers including clear cell component had better survival compared with those with pure CCC [18]. Additionally, a report demonstrated that diagnosis of mixed epithelial ovarian cancers with clear cell component was not reproducible [26]. Central pathologic review used in the present study might have excluded mixed epithelial cancers with clear cell component which potentially have better prognosis compared with pure CCC. Additionally, there is a report describing a significant worse post-recurrent survival in CCC compared with that in SAC [27]. The worse post-recurrent survival could have led to extremely worse OS in patients with CCC.
In the present study, chemotherapeutic regimen was not a prognostic factor for PFS or OS in stage II-IV CCC. The gold standard regimen for ovarian cancer has been a combination with paclitaxel and carboplatin (TC). This regimen has been used widely for all histological subtypes of epithelial ovarian carcinoma, including CCC. However, only 2-5% of the patients were enrolled in these randomized trials had CCC histology [6,28,29]. As a candidate for primary chemotherapy for CCC, a combination with irinotecan and cisplatin (CPT-P) showed equivalent PFS and tolerability to TC [30]. A randomized clinical trial, GCIG/JGOG3017 [31], comparing CPT-P and TC for primary therapy of CCC, will show us whether an individualized chemotherapy based on histologic subtype is helpful in the treatment of CCC.
In conclusions, in stage I ovarian cancers, clear cell subtype was not a prognostic factor but peritoneal cytology was. PFS and OS of advanced CCC patients were significantly poorer than those of SAC cases, and histology of CCC was an independent prognostic factor in advanced ovarian cancers. These results should be taken into consideration for further clinical studies.




 XML Download
XML Download