

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Among gynecologic malignancies, ovarian cancer is the leading cause of cancer-related deaths [1]. The International Federation of Gynecology and Obstetrics (FIGO) staging for ovarian cancer reflects the prognosis of affected patients. The current staging was accepted by FIGO in 1988. However, many studies have indicated the necessity of a revision of the current FIGO staging guidelines for better prognostic discrimination. For stage IC disease, a growing body of evidence suggests that intraoperative rupture might not increase the risk of tumor recurrence [2,3]. For stage IIB disease, macroscopic pelvic peritoneal tumor masses might be associated with poor survival outcomes compared with microscopic tumor infiltration or adherence [4]. Many studies have reported better prognosis for stage IIIC ovarian cancer with lymph node (LN) involvement alone (without peritoneal carcinomatosis) than with LN involvement and concomitant peritoneal carcinomatosis [5-7]. The revision process is currently underway by the Gynecology Oncology Committee of FIGO in collaboration with various international societies and agencies, and the revision would be addressed about the stage IIIC classification, at least [8].
Since the revision process should be finalized only after a consensus is reached by all relevant international organizations through extensive consultations, we performed this timely study to evaluate whether the revision of FIGO sub-staging for ovarian carcinoma could improve prognosis prediction. Furthermore, the favorable prognosis of FIGO stage IIIC ovarian cancer characterized by LN-positive disease only, prompted us to compare the survival outcomes of stage IV disease so-assigned based on supraclavicular LN metastasis with those of stage IV disease so-assigned based on the other metastatic sites.
MATERIALS AND METHODS
Data were obtained from the review of the medical charts of all patients with epithelial ovarian, fallopian tube, and primary peritoneal cancers at three Seoul National University-affiliated hospitals between 1990 and 2011. Each of the Institutional Review Boards of the three hospitals approved this study. Data on patient demographics, primary cancer sites, stages, grades, histology, first courses of treatment, intraoperative findings regarding tumor spread, operation procedures performed, residual disease, adjuvant chemotherapy, recurrence, and survival were collected. Optimal cytoreduction was defined as a residual tumor size of <1 cm. A total of 870 patients were eligible for analysis, as shown in Fig. 1.
Stages were reassigned according to the following criteria when indicated: surgical spillage with intraoperative tumor rupture (IC1), capsule rupture before surgery or presence of a tumor on the surface (IC2), and presence of malignant cells on ascites or peritoneal washing cytology (IC3); microscopic (IIB1) and macroscopic (IIB2) pelvic spread; microscopic extrapelvic spread (IIIA1) and retroperitoneal LN metastasis without extrapelvic spread (IIIA2); and supraclavicular LN metastasis (IVA) and other distant metastasis (IVB).
Kaplan-Meier survival estimates were derived for overall survival (OS) both before and after stage reassignment. Univariate and multivariate analyses were performed using Cox proportional hazards models in order to evaluate the association between the site of distant metastasis and OS outcomes. Various prognostic factors for the sub-stages were also compared using the chi-square test, Student's t-test, and Kruskal-Wallis test, as appropriate, to assess the association of these factors with survival outcomes. The OS rates were defined as duration from the date of diagnosis to either the recorded date of death from ovarian cancer or the date of death provided by Statistics Korea. Statistical tests were 2-sided, with p<0.05 indicating significance. Statistical analyses were performed using SPSS ver. 19.0 (IBM Co., Armonk, NY, USA).
RESULTS
The median follow-up period was 45 months (range, 0 to 263 months). Characteristics of the study population are summarized in Table 1. Stage migrations after stage reassignment and the corresponding 5-year OS rates (5YSR) are described in Table 2.
1. Stage IC
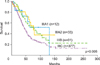
The 5YSR for patients with stage IC disease (n=119) was 82.5%. After stage reassignment, the 5YSRs of patients with sub-stage IC1 (n=39), IC2 (n=27), and IC3 (n=53) disease were 92.0%, 85.0%, and 71.0%, respectively (p=0.004) (Fig. 2). Age, initial serum CA-125 level, tumor grade, lymphadenectomy rate, use of taxane-platinum-based adjuvant chemotherapy, and completion of chemotherapy ≥6 cycles did not differ according to sub-stage. Although patients who were assigned an advanced sub-stage had a higher frequency of serous cancer than those with early sub-stage disease did (p=0.02), multivariate analysis using Cox proportional hazards models revealed that serous-type cancer was not an independent prognostic factor for OS (p=0.766).
We performed additional analysis in the patients (n=64) who underwent staging operation along with lymphadenectomy, considering the low rate of lymphadenectomy in the patients with early stage disease. There were 20 IC1, 15 IC2, and 29 IC3 patients after stage reassignment. We found a significant OS difference among the patients according to the three sub-stages in this subset (p=0.021).
2. Stage IIB
The 5YSR for patients with stage IIB disease (n=32) was 75.0%. After stage reassignment, the 5YSRs of patients with sub-stage IIB1 (n=11) and IIB2 (n=21) disease were 70.0% and 76.0%, respectively (p=0.461) (Table 2).
3. Stage III
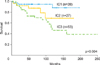
The 5YSR for patients with stage IIIC disease (n=410) was 38.5%. However, after stage reassignment, the 5YSR of patients with sub-stage IIIA2 disease (n=33) was significantly higher than that of the remaining patients with stage IIIC disease (n=377) who had extrapelvic tumors >2 cm (66.3% vs. 35.8%; p=0.005) (Fig. 3), and even higher than that of patients with sub-stage IIIA1 disease (57.5%) (Table 2). The rate of optimal cytoreduction was significantly higher in stage IIIA2 disease than in stage IIIC disease (p=0.006). Lymphadenectomy was performed more frequently in the patients with stage IIIA2 disease than in those with stage IIIC disease (p<0.001). However, patients with stage IIIA2 and IIIC disease did not show any difference in age, initial serum CA-125 level, serous histology, tumor grade, neoadjuvant chemotherapy rate, use of taxane-platinum based adjuvant chemotherapy, and receipt of ≥ 6 chemotherapy cycles. Multivariate analysis using Cox proportional hazards models revealed that optimal cytoreduction was an independent prognostic factor for OS in stage III disease (hazard ratio [HR], 2.1; 95% confidence interval [CI], 1.6 to 2.7; p<0.001).
4. Stage IV
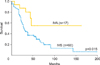
The 5YSR for the patients with stage IV disease (n=77) was 33.0%. After stage reassignment, the 5YSRs of the patients with sub-stage IVA (n=17) and IVB (n=60) disease were 52.0% and 28.0%, respectively (p=0.015) (Fig. 4). Age, initial serum CA-125 level, serous histology, tumor grade, neoadjuvant chemotherapy rate, rate of optimal cytoreduction, lymphadenectomy rate, use of taxane-platinum-based adjuvant chemotherapy, receipt of ≥6 chemotherapy cycles, and the rate of chemoresistance did not differ between patients with the 2 sub-stages. Nevertheless, chemoresistance (HR 7.4; 95% CI, 2.8 to 19.3; p<0.001), no use of taxane-platinum based adjuvant chemotherapy (HR, 35.4; 95% CI, 1.7 to 733.4; p=0.021), and receipt of <6 chemotherapy cycles (HR, 17.7; 95% CI, 4.3 to 72.3; p<0.001) were independent poor prognostic factors for OS in stage IV ovarian cancer (data not shown). Table 3 shows the results of univariate and multivariate survival analyses for stage IV ovarian cancer, according to the site of distant metastasis. There was no case of spleen parenchymal metastasis in our study population. Although patients with brain metastasis had the longest median OS, multivariate analysis using Cox proportional hazards models revealed that supraclavicular LN metastasis was an independent favorable prognostic factor for OS with regard to the site of metastasis in ovarian cancer (HR, 0.22; 95% CI, 0.08 to 0.63; p=0.005). In contrast, bone metastasis was an independent prognostic factor for poor OS (HR, 3.49; 95% CI, 1.10 to 11.08; p=0.034). Compared with the lung, bone, and brain metastases, which frequently showed multiple metastatic lesions, supraclavicular LNs often showed single one.
DISCUSSION
Our study demonstrates the necessity for revision of the current FIGO staging for ovarian cancer with regard to the 3 sub-staging issues for stages IC, III, and IV. The sub-staging process has 2 main implications. First, stage IC was sub-staged as stages IC1, IC2, and IC3, to account for the distinct prognoses associated with the etiology of tumor rupture. Second, considering the relatively favorable prognosis associated with lymphatic tumor spread compared with peritoneal tumor spread, stage IIIC, which was classified solely on the basis of LN metastasis, was down-staged to stage IIIA2. Similarly, stage IV was sub-staged as stage IVA, with distant metastasis to the supraclavicular LNs, and stage IVB, with other distant metastasis.
There has been much controversy regarding the cause of tumor rupture that upstages cancers to stage IC with regard to prognosis. Vergote et al. [9] demonstrated that tumor rupture during surgery (HR, 2.65; 95% CI, 1.53 to 4.56; p<0.001) and before surgery (HR, 1.64; 95% CI, 1.07 to 2.51; p=0.022) had an independent unfavorable impact on disease-free survival. However, other researchers failed to show that capsular rupture caused by the surgeon affected the prognosis of patients with early-stage ovarian cancer [3,10,11]. A recently published meta-analysis supported this finding and concluded that intraoperative rupture might not decrease progression-free survival compared to no rupture in early-stage ovarian cancer with complete surgical staging and adjuvant platinum-based chemotherapy [2]. This finding is consistent with our findings that the 5YSR of patients with sub-stage IC1 disease was similar to that of patients with stage IA disease and was clearly higher than that of patients with sub-stage IC3 disease.
Many studies have supported Berek's suggestion of a separate entity for LN-positive stage IIIC ovarian cancer [5-7]. Berek [5] argued that FIGO should consider modifying the ovarian cancer staging by further stratifying stage III disease on the basis of the better OS in patients with retroperitoneal LN metastasis without peritoneal carcinomatosis than in patients with macroscopic peritoneal carcinomatosis. One plausible explanation for the favorable prognosis of those patients with sub-stage IIIA2 disease might be the higher optimal cytoreduction rate compared to the patients with stage IIIC disease showing intraperitoneal tumor implants >2 cm. Optimal cytoreduction was a well-known and important prognostic factor for advanced-stage ovarian cancer [12]. Our study also showed that optimal cytoreduction was an independent prognostic factor for OS in patients with stage III disease. Bachmann et al. [13] reported that the influence of LN metastasis on prognosis decreases with the increase in residual tumor volume. The authors also reported that the nodal status seemed to be the next most important prognostic factor for advanced-stage ovarian cancer. Additionally, successful retreatment of recurrence in patients upstaged to stage IIIC on the basis of LN metastasis alone with second surgery and chemotherapy could partly account for the favorable prognosis of these patients [6,14,15].
The primary routes of ovarian cancer metastasis include intra-peritoneal implantation of exfoliated cells at distant sites and spreading through retroperitoneal lymphatic channels [16]. Spreading through the lymphatic channels of the diaphragm and the retroperitoneal LNs can lead to dissemination above the diaphragm, especially to the supraclavicular LNs [5]. In accordance with the favorable prognosis of LN-positive-only stage IIIC disease, stage IV disease, assigned on the basis of supraclavicular LN metastasis, might be associated with better survival outcomes than stage IV disease. Nevertheless, no study has investigated the favorable prognosis of stage IV ovarian cancer patients with supraclavicular LN metastasis. To the best of our knowledge, this study is the first one to demonstrate a distinctly better OS for stage IV ovarian cancer patients with supraclavicular LN metastasis than for patients with other forms of distant metastasis. Since ovarian cancer is known to spread both intraperitoneally and retroperitoneally almost simultaneously [17], the presence of tumor spreading mainly through lymphatic channels without intra-peritoneal dissemination suggests that such tumors might be associated with a favorable biologic behavior. In support of this idea, our study shows that sub-stage IVA disease was associated with a relatively limited number of simultaneous metastatic sites compared with sub-stage IVB disease. However, in this study, we failed to show any significant positive or negative associations between the prognosis of patients with sub-stage IVA disease and the prognostic factors that were already proven important for advanced-stage ovarian cancer, such as optimal cytoreduction and chemoresistance.
This study has some limitations. First, we did not show a significant difference in OS between sub-stages IIB1 and IIB2. This might be partly due to the small number of patients with stage II disease. FIGO stage II ovarian cancer accounts for 8% of all ovarian cancers [4] and 6.4% in our study. Further studies with larger population numbers are needed in order to achieve sufficient statistical power. Second, the follow-up period for the study population was relatively short. This might result in an overestimation of the favorable prognosis of patients with stage IVA disease (5YSR, 52.0%), which was even better than that of patients with stage IIIC disease. A longer follow-up period could ensure that the survival estimates are more accurate. Third, the low rate of lymphadenectomy in early stage disease implicated that true pathologic stage IIIC disease could be included in the analysis of stage IC disease. However, the same result of a significant OS difference in stage IC patients who underwent staging lymphadenectomy was observed. Finally, mortality was not disease-specific but overall, without considering the cause of death. This might cause an underestimation of prognosis in this study. Nevertheless, the potential impact of this underestimation on the study results could be minimal because the age difference between the compared sub-stages was not significant.
In conclusion, modification of the current FIGO staging for ovarian carcinoma appears to improve the discrimination of the survival outcomes of patients with surgical spillage, retroperitoneal LN metastasis without extrapelvic peritoneal involvement, or distant metastasis to the supraclavicular LN. Further studies are warranted to explore the biologic mechanisms that underlie the favorable prognosis of patients with stage IV disease, so-assigned on the basis of supraclavicular LN metastasis.



 XML Download
XML Download