

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer is the second most common gynecologic malignancy in the world. The major steps required for cervical carcinogenesis include human papillomavirus (HPV) infection, HPV persistence, progression to precursor lesions, and invasion [1]. The majority of cervical cancer cases are caused by persistent infection with at least one of the high-risk (HR) carcinogenic HPV types [2]. Consequently, it has been proposed that, like the HPV DNA test, highly sensitive HPV detection methods may be able to strengthen the efficacy of population-based screening programs, either as a sole screening tool or as an adjunct to current cervical cancer triage. Hybrid Capture 2 (HC2, Qiagen, Gaithersburg, MD, USA), mostly used as an HPV detection method, can detect the DNA of the 13 HR and 5 low-risk HPV types that most commonly affect the cervix. However, HC2 is unable to determine specific HPV types, and HPV 16 and HPV 18 genotypes are responsible for causing the majority of all cervical cancers [3]. Thus, another method is necessary for specific HPV genotyping.
Recently, two novel DNA test methods for HPV detection and genotyping have been developed, Seeplex HPV4A ACE (Seegene Inc., Seoul, Korea) and the Cervista HPV assays (Hologic Inc., Madison, WI, USA). In contrast to other commercially available HPV genotyping methods, Seeplex HPV4A ACE is DPO-based multiplex PCR. HPV 16 and/or 18 genotyping and 16 HPV HR type and HPV low risk HPV 6/11 screening can be done with one PCR test. The Cervista HPV HR and 16/18 tests uses the Invader chemistry (Hologic Inc.), a signal amplification method for detection of specific nucleic acid sequences. The Cervista HPV HR is designed for detection of 14 HPV types. This method uses two types of isothermal reactions, including a primary reaction that occurs on the targeted DNA sequence and a secondary reaction that produces a fluorescent signal.
The Cerivsta HPV assays must be conducted separately, but Seeplex HPV4A ACE is so robust that physicians can obtain HPV results in a single test. The purpose of this study was to validate the sensitivity of Seeplex HPV4A ACE for the detection of HR HPV DNA and HPV 16 and/or HPV 18 genotypes, as compared to the PCR method, the Cervista HPV HR, and Cervista HPV 16/18, in cervical swab samples. Finally, we evaluated the sensitivity and specificity of these HPV DNA tests in correlation with cytologic results.
MATERIALS AND METHODS
1. Study population, specimen collection, and histologic examination
Women were enrolled who were referred to the Colposcopy Clinic in Korea University Guro Hospital due to abnormal cytology between April and June 2010. A cervical specimen for liquid-based cytology, along with simultaneous HPV DNA detection by the HC2 assay, was collected from each patient. Genomic DNA was extracted from each sample, and the HPV DNA tests were performed by HPV4A ACE, PCR method, Cervista HPV HR assay, and Cervista HPV 16/18 test on the same specimen. Among them, we used only samples of HPV-positive women by HC2 assay due to the difficulty of HC2-negative sample collection as limitation of this retrospective study. Colposcopic examinations were performed in all women with abnormal cervical cytology. Histologic verifications by punch biopsy were performed in women with abnormal colposcopic findings.
2. Liquid-based cytology
A Cervex-Brush (Rovers Medical Devices, Oss, Netherlands) was used to obtain samples from the uterine cervix. The brush was immediately rinsed in a vial of PreservCyt solution (Hologic Inc.). The vial was placed in the ThinPrep Processor (Hologic Inc). The ThinPrep slide was then fixed in ethanol and stained with Papanicolaou's stain. The number of epithelial cells on these slides was estimated from the number of cells contained within computer-derived coordinates for 50 random fields located within a 20-mm diameter circular area where the cells were deposited. The diagnoses were made using the 2001 Bethesda System for cervical cytology.
3. HC2 assay
HPV DNA testing by the HC2 assay was performed with the HC2 assay system according to the manufacturer's protocol (Qiagen). The specimens were denatured at 65℃ for 45 minutes and hybridized under high-stringency conditions with a mixture of RNA probes that detects 13 different oncogenic HPV types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. The resultant DNA-RNA hybrids were captured on the surface of the microtiter plate wells coated with an anti-DNA-RNA hybrid antibody. The immobilized hybrids were then reacted with an alkaline phosphatase-conjugated antihybrid monoclonal antibody. Light intensity was measured with a luminometer. The recommended positivity threshold of 1 pg/mL was used as a cutoff, and all specimens with a relative light unit/control (RLU/CO) ratio of ≥1.0 were considered positive.
4. PCR method
PCR was conducted in a final reaction volume 20 µL containing 0.1 µg of isolated DNA from a cervical swab, 1 µL of forward (F) and reverse (R) primer (General (F): 5'-TTTGTTACTGTGGTAGATACTAC-3', General (R): 5'-GAAAAATAAACTGTAAATCATATTC-3', HPV 16 (F): 5'-TTTGTTACTGTTGTTGATACTACACGC-3', HPV 16 (R): 5'-GAAAAATAAACTGTAAATCATATTCCTC-3', HPV 18 (F): 5'-TTTGTTACTGTGGTAGATACCAC TCGC-3', HPV 18 (R): 5'-GAAAAATAAACTGCAAATCATATTCCTC-3', 10 pmole/µL) and 10 µL of 2X Master Mix (Lucigen, Middleton, WI, USA). Here, general primers were common primers to confirm HR HPV. After a pre-heating step at 94℃ for 4 minutes, 40 amplification cycles were carried out in the thermal cycler under the following conditions: denaturation at 94℃ for 1 minutes, annealing for 2 minutes and extension at 72℃ for 90 seconds. Amplification was completed with a final extension step at 72℃ for 4 minutes. The amplified PCR products were separated on 4% agarose gel containing ethidium bromide.
5. Seeplex HPV4A ACE screening
Seeplex HPV4A ACE is designed for detection of HPV 16 and/or HPV 18, screening for 16 HPV HR types (i.e., 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73 and 82), and screening for HPV low risk types 6/11. The residual cells in the PreservCyt solution were centrifuged at 13,000 ×g for 15 minutes, and the cell pellets were resuspended in 100 µL of phosphate-buffered saline. The resuspended cell pellets were added to a Qiamp DNA mini Kit (Cat. No. 51304, Qiagen Inc., Valencia, CA, USA). The extraction of total DNA was performed according to the manufacturer's instructions. HPV DNA testing by the Seeplex HPV4A ACE was performed according to the manufacturer's protocol (Seegene, Korea). The kit contains sets of primers that were specifically designed from highly conserved regions of genetic sequences for HPVs using DPO technology [4]. Optimized multiplex PCR was performed in 20 µL reactions containing DNA template, primer mixture, 2X Master Mix (Seegene, Korea) and 8-methocypsoralen (MOP), which prevents contaminating DNAs for being amplified. PCR amplification was performed in an Applied Biosystem 9700 thermal cycler (Perkin-Elmer, Boston, MA, USA) with the following conditions: After a pre-heating step at 94℃ for 15 minutes, 40 amplification cycles were carried out in the thermal cycler under the following conditions: denaturation at 94℃ for 30 seconds, annealing at 60℃ for 90 seconds, and extension at 72℃ for 90 seconds. Amplification was completed with a final extension step at 72℃ for 10 minutes. The amplified PCR products were separated on an auto capillary electrophoresis system, the LabChip DX Seeplex Assay system (Caliper, Hopkinton, MA, USA).
The PCR products from each sample (20 µL) were transferred to a 96 well plate and placed in the LabChip DX instrument. The samples were loaded automatically on the Seeplex Chip and detected sequentially according to the sample order. Analysis was performed with designated software (Seegene viewer) that presents each of the samples and identifies the fragments that yield a positive readout for the bands of interest in the presented results. A tabulated matching matrix provides a simple readout, identifying matching bands to the types of HPV. A text file is automatically generated and saved for each tape.
6. Cervista HPV HR test and Cervista HPV 16/18 test
The Cervista HPV HR is designed for detection of 14 HPV types (i.e., types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68). The DNA was extracted from residual liquid cytology samples that contained at least 2 mL of sample volume, using the Genfind DNA Extraction Kit (Third Wave Technologies Inc./Hologic Inc., Madison, WI, USA), to perform the HR HPV and 16/18 genotyping tests. DNA was extracted twice, from 2 mL aliquots of the original sample, and placed into 2 separate cryovials labeled B and C. Cryovial B was used for analysis of HR HPV and 16/18 genotyping. Cryovial C was retained for long-term storage except when required as backup material. The technology for the HR HPV and 16/18 genotyping tests has been previously described [5].
7. Statistical analysis
To compare the clinical accuracy of Seeplex HPV4A ACE and the Cervista HPV HR test to detect lesions higher than low-grade squamous intraepithelial lesions (LSIL), we also calculated the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV); the sensitivity and specificity of the two tests were compared by the receiver operating characteristic (ROC) curve in dbSTAT for Windows (dBSTAT, Seoul, Korea). Agreement between the HPV assays was assessed by Cohen's κ statistic, with values of 0.00-0.20 indicating poor agreement, 0.21-0.40 fair agreement, 0.41-0.60 moderate agreement, 0.61-0.80 substantial agreement, and 0.81-1.00 almost perfect agreement. In addition, we used the dbSTAT for Windows to compare the predictive values between the HR HPV-targeted method and HPV 16 and/or 18-targeted methods. Statistical analyses were performed with SPSS ver. 19.0 (IBM Co., New York, NY, USA) and dBSTAT for Windows ver. 4.5 (dBSTAT). All tests were 2-sided, and a P value of less than 0.05 was considered significant.
RESULTS
The cytologic findings, as well as all three HPV DNA test results, were available for 197 patients. The positive rates of each HPV DNA test were 52.3% (103/197) by PCR method, 45.7% (90/197) by Seeplex HPV4A ACE, and 44.2% (87/197) by the Cervista HPV HR test (Table 1). The HR HPV-positive rates by PCR, Seeplex HPV4A ACE, and the Cervista HPV HR test were 11.0%, 4.0%, and 6.0% for the normal cytology group; 89.7%, 84.6%, and 82.1% for atypical squamous cells (ASC); and 98.2%, 91.4%, and 84.5% for detection of lesions of more than LSIL, respectively.
The concordance for HR HPV detection between the Cervista HPV HR test and PCR was 81.7%, showing substantial agreement (κ coefficient=0.636) (Table 2). Additionally, the concordance between Seeplex HPV4A ACE and the Cervista HPV HR test was 87.3%, showing substantial agreement (κ coefficient= 0.744). For the detection of HPV 16 and/or 18, Seeplex HPV4A ACE and the Cervista HPV 16/18 test showed substantial agreement (89.5%, κ coefficient=0.628).
Table 3 shows the diagnostic accuracy of each HPV DNA test related to cytologic results. The overall HR HPV prevalence was increased in parallel with the increasing severity of the Pap smear result. When an abnormal Pap test was defined as ASCs of undetermined significance (ASCUS) or higher, the sensitivity and specificity of Seeplex HPV4A ACE and Cervista HPV HR both had high test results. However, Seeplex HPV4A ACE definitely showed a higher sensitivity and specificity compared to Cervista HPV HR (88.7% vs. 83.5% and 96% vs. 94%, respectively) (Table 3). However, no statistical difference was observed between the two tests. Likewise, when the abnormal Pap test was defined as LSIL or higher, the two HPV DNA tests showed no difference for the detection of cytological results.
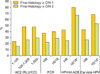
We calculated the predictive value for cervical intraepithelial neoplasias (CINs) of each HPV test according to cervical histology (Fig. 1). In HC2, the predictive value for CINs tended to increase with the level of viral load. However, it was difficult to identify the exact cutoff value to detect CINs. In the other HPV genotyping tests, Seeplex HPV4A ACE, and Cervista HPV assays, methods to target HPV 16 and/or 18 had a higher predictive value than that of HR HPV (66.7% vs. 24.6% by HPV4A ACE, 52.6% vs. 25.9% by Cervista HPV assays in CIN II or more, relatively, p<0.05).
DISCUSSION
In this study, we found a high efficacy of Seeplex HPV4A ACE in detecting HR HPV, HPV 16, and HPV 18 compared with the PCR method and Cervista HPV HR and HPV 16/18 tests in HC2-positive cervical samples.
The most obvious cause of cervical precursor lesions or cancer is persistent infection with one of the carcinogenic HPVs [3]. Among those HPVs, the proportion of HPV types 16 and 18 is the greatest in the development of CIN or cervical cancer [3]. It has been shown that women positive for HPV 16 and HPV 18 have an increased risk of high-grade CIN compared with women positive for other HR HPV types [6-9]. For this reason, it is important to distinguish HPV 16 and HPV 18 among the carcinogenic HPV types.
The Cervista HPV HR is designed to detect all 14 oncogenic HPVs and to reduce false-positive results caused by cross-reactivity with low-risk HPV genotypes using signal amplification and fluorescence detection. In addition, the Cervista HPV HR contains a unique internal control to validate that sufficient DNA is present for testing. The Cervista HPV 16/18 test, which genotypes for HPV 16/18, is built on same method as Cervista HPV HR. Since then, the results of studies regarding the efficacy of Cervista HPV HR and HPV 16/18 have been presented by several researchers [5,10-12]. The Seeplex HPV4A ACE test can detect 18 HR HPV genotypes. Among these, the common primers of HR HPV may detect HPV types 39, 52, and 68 by cross-reactivity. Seeplex HPV4A ACE demonstrated substantial agreement with PCR (88.3%, κ=0.767). Despite the fact that Seeplex HPV4A ACE has not yet been approved by the FDA, the efficacy of this test is superior over any other products as published previously [13]. This proves the simplicity and reliability of HPV4A ACE for HPV genotyping and screening. If two tests have similar abilities to predict abnormal cytology or more than CIN II lesions as in our results, it is more useful to patients and physicians to use a method that can genotype and screen in one test.
In this study, we consider the HC2 assay as the gold standard for HR HPV detection, and Seeplex HPV4A ACE and the PCR method as a comparative study for HPV 16/18 genotyping. After the HC2 assay was approved first by the FDA in 2003, it was used as the gold standard in recently published articles regarding HPV DNA tests [13-17]. Unfortunately, HC2 can only detect the presence of 13 types of HR-HPV. To apply this test in an actual clinical situation, it is considered more useful to compare its results to those of another currently used method. For this reason, we decided to use Seeplex HPV4A ACE and PCR for genotyping as the real-time PCR technique can reinforce the weakness of HC2. Other limitations of this study are that this study did not include a negative result of HC2 and that this study was conducted retrospectively. In a study conducted by Digene and the National Cancer Institute, an overall 82.8% agreement (173/209; 95% confidence interval [CI], 77.0 to 87.6) was observed between HC2 and PCR and a positive and negative agreement of 96.7% and 44.6%, respectively (95% CI, 92.5 to 98.9 and 31.3 to 58.5). Due to the possibility of false positive results of HC2, we should include HC2-negative samples for an accurate analysis. However, as mentioned in Materials and Methods, HC2-negative samples are difficult to collect due to the limitation of this retrospective study. So, we took to experiment with the HC2-positive samples, but, because of the high overall and positive agreements, we decided to offset the impact that may occur to conduct research on HC2-positive samples only.
Seeplex HPV4A ACE has the ability to detect the presence of 18 HR HPV genotypes in high concordance with PCR simultaneously, and it also can identify HPV 16 and/or 18 genotypes similar to the Cervista HPV HR test. Seeplex HPV4A ACE has not yet received FDA-approval, but it could be said with sufficient means as a HPV DNA test. HPV genotyping tests for HPV 16/18 should be considered to detect CINs more accurately. Seeplex HPV4A ACE is strongly recommended for the detection of HR HPVs and for genotyping of HPV 16 and/or 18. Continuous studies with larger numbers of samples and comparison data with other various HPV DNA genotyping methods are necessary to make this novel diagnostic tool more credible and practical at the same time. Research is needed that compare HPV DNA tests by including all of the HC2 results and serial tests on the same target group.


 XML Download
XML Download