

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) is the second most common gynecologic malignancy in developed countries, and accounts for more deaths than the remaining gynecologic cancers added together [1]. EOC can spread by intraperitoneal seeding, direct invasion, or through lymphatic or vascular circulation, and the peritoneal seeding is the most common route of dissemination [2].
In most women with EOC, the disease is not diagnosed until it is at an advanced stage. Primary cytoreductive surgery followed by taxane/platinum-based adjuvant chemotherapy is considered the standard approach to these patients [3]. Some observers have noted that the maximal cytoreduction, correlated to the minimal residual tumor mass after surgery, is one of the most powerful prognostic factors [4-6].
Imaging of the peritoneum has been routinely performed by means of contrast-enhanced CT, however, the sensitivity of this technique depends on the size and location of peritoneal implants. Moreover, anatomical imaging uses only size criteria and does not recognize the functional alterations that occur within tumor tissue. PET/CT using [18F]FDG has been successfully employed to visualize enhanced glucose utilization in tumor tissues. PET/CT has been shown to identify primary tumors, regional lymph nodes, and distant metastases with high diagnostic accuracy for primary and recurrent EOC [7-10]. These hybrid systems perform both PET and CT and co-register images with an improvement of anatomic localization of intra- and extra-pelvic structures [11], as well as allowing the detection of distant supra-diaphragmatic metastases [12]. Several studies have shown that PET or PET/CT were useful for monitoring treatment response [13,14], detecting residual disease after completion of therapy [15,16], and detecting recurrent or metastatic lesions in EOC [8,17].
However, only limited information is currently available describing the role of PET/CT for the prediction of recurrence in EOC. This study evaluated the hypothesis that the pretreatment metabolic activities measured by FDG uptake and its distribution will allow prediction of prognosis. The aim of this study was to evaluate the prognostic value of the distribution of FDG uptake on preoperative PET/CT scans in patients with EOC.
MATERIALS AND METHODS
1. Patient population
This study was approved by our institutional review board. We retrospectively reviewed the tumor registry at our institution and identified all patients diagnosed with EOC between January 2004 and December 2009. All clinical, histological and imaging data of patients at our institution were collected and stored in a computerized database. Patients were required to have undergone an PET/CT study just before establishing a pathologic diagnosis, to have received no treatment before the study, and to have had at least 3 months of follow-up.
Patients were excluded in the analysis if any of the following criteria were present: 1) a previous diagnosis of another malignant disease or borderline tumor, 2) short follow-up duration less than 3 months, 3) primary treatment other than surgery such as neoadjuvant chemotherapy, 4) known allergy to contrast media, diabetes or other severe medical conditions. Tumor histologic cell type, grade, stage at surgical staging, site of metastasis, and treatment were recorded from the patient's medical record. A stage after surgical staging was assigned according to the International Federation of Gynecology and Obstetrics (FIGO).
2. PET/CT imaging
The patients were imaged using a dedicated PET/CT system (Gemini, Philips Medical Systems, Andover, MA, USA). All patients were instructed to fast at least 4 hours prior to undergoing PET/CT; 125 mL of a barium sulfate solution (Readi-cat [1.3% weight-volume barium sulfate suspension]; E-Z-EM, Westbury, NY, USA or EZCT [1.5% weight-volume barium sulfate suspension], Taejoon Pharm, Seoul, Korea) was administered orally 1 hour prior to imaging to opacify the bowel for the CT portion of the study, following methods described in our previous study [18]. PET/CT scans were obtained between 1 day and 23 days (median, 5 days) before surgery.
3. Image analysis
All images were interpreted and analyzed by two experienced nuclear medicine physicians (HWK, KWK) with all available clinical information. The images were reviewed on an interactive video display provided by the equipment manufacturer standardized uptake value (SUV)location was quantitatively used to determine FDG activity. Calculation of SUVmax was as follows: SUVmax = Cmax×TBW/IA (Cmax, activity concentration in the voxel of highest metabolic activity [Bq/mL]; TBW, total body weight (kg); IA, injected activity [kBq]).
SUV distribution was divided into two regions at the level of the umbilicus, and the impact of the ratio between above and below the umbilicus (SUVlocation ratio = sum of SUV above umbilicus / sum of SUV below umbilicus) on recurrence was examined.
4. Treatment and follow-up
After the PET/CT scan and a definitive surgical staging, 50 patients were treated with chemotherapy. Survival data were obtained from the tumor registry and verified on review of the medical records.
5. Histological and clinical evaluation
Recurrent disease was confirmed in all cases by either tissue biopsy or the demonstration of progressive disease by serial imaging studies such as CT, MRI, or PET/CT. Clinical proof of no recurrent disease consisted of a negative tissue biopsy and negative finings on serial follow-up imaging studies.
To confirm lesions detected on PET/CT imaging, CT- or ultrasound-guided biopsy was performed to obtain tissues for histological evaluation in cases where it was considered necessary for patient management. Progressive elevation of serum tumor marker (CA-125) accompanied by an increase in lesion size or the appearance of new lesions was considered disease recurrence.
6. Data analysis
With respect to SUVlocation ratio, receiver operating characteristic (ROC) curve analysis was performed in order to determine the cutoff values for predicting recurrence. Progression-free survival (PFS) was calculated as the interval from the date of treatment completion to the first documented date of progression, or death whichever occurred first. Survival curves were constructed using the method of Kaplan and Meier. The Cox proportional hazards modeling used to identify independent variables associated with recurrence. Results from the Cox models are expressed as hazard ratios (HRs) with 95% confidence intervals (CIs), and p<0.05 was considered the level of significance. The SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis.
RESULTS
1. Characteristics of the patients
Of the 337 patients diagnosed as EOC, 299 patients underwent primary debulking surgery during the study period. There were 76 patients with a median age of 54 years (range, 35 to 80 years) who met the inclusion criteria. A total of 55 patients underwent preoperative PET/CT scanning.
2. PET/CT and survival
Median follow-up time was 16 months (range, 3 to 50 months), and the median PFS duration was 11 months (range, 3 to 43 months). Twenty (36.4%) patients experienced recurrence, and one patient died of disease. The 3-year PFS rate was 50.8%.
3. Cutoff value of SUVlocation ratio
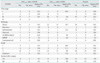
Fig. 1 shows the ROC curve analyzing the SUVlocation ratio in PFS. Area under the curve (AUC) was 0.740 (p=0.004; 95% CI, 0.607 to 0.873), and the value of 0.3934 was determined as the cutoff of SUVlocation ratio in this study, and patients were categorized into two groups according to the SUVlocation ratio (<0.3934 vs. ≥0.3934). Table 1 lists the descriptive statistics among demographic subgroups categorized by the cutoff SUVlocation ratio. Patient distribution was significantly different according to FIGO stage (p=0.015), residual disease after surgery (p=0.017), and patients status (p=0.004) between the two groups categorized by the SUVlocation ratio. Table 2 lists the median PFS among groups categorized by the cutoff SUVlocation ratio.
4. SUVlocation ratio and recurrence
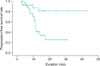
Table 3 shows the results of the Cox proportional hazard analyses. In univariate analysis, high SUVlocation ratio (p=0.002; HR, 1.974; 95% CI, 1.286 to 3.031) was significantly associated with recurrence. Malignant mixed mullerian tumors (MMMT) compared with endometrioid histology was also shown to have significance. In multivariate analysis, high SUVdistribution ratio (p=0.005; HR, 2.418; 95% CI, 1.1315 to 4.447), and histology (serous, p=0.031; mucinous, p=0.045; MMMT, p=0.003; compared with endometrioid type) were significantly associated with recurrence. The Kaplan-Meier survival graph showed a significant difference in PFS between the groups categorized by SUVlocation ratio (Fig. 2). Survival difference between the two groups was statistically significant (p=0.0021, log-rank test).
DISCUSSION
The purpose of the current study was to determine whether the preoperative metabolic tumor burden and its distribution as measured by the SUV have prognostic significance in patients with EOC. To the best of our knowledge, this is the first study reporting the prognostic value of preoperative PET/CT on predicting the risk of recurrence in patients with EOC.
The principle finding was that the metabolic tumor burden in the upper abdomen measured as SUVlocation ratio on preoperative PET/CT was the most powerful significant prognostic factor for predicting recurrence in EOC. It is noteworthy that FIGO stage was not a significant prognostic factor for recurrence in this study. This may be due to the small number of patients enrolled, and the distribution of stage (most patients were stage III). We found that another tumor-related factor such as tumor histology was also a predictor of recurrence.
The results of the current study demonstrate the potential value of preoperative PET/CT in patients with preoperative SUVlocation ratio. We aim to perform more frequent and intensive follow-up or prophylactic administration of consolidation treatment in these patients, and may individualize patient care according to the preoperative SUVlocation ratio.
In previous studies, the presence of residual tumor after primary surgery has been shown to be an independent prognostic factor [19-23]. A Gynecologic Oncology Group (GOG) study demonstrated that patients with stage III disease presenting with large-volume ovarian cancer before undergoing optimal cytoreduction had a worse prognosis than patients found to have small-volume disease at the time of exploration [24]. The Scottish Randomized Trial in Ovarian Cancer (SCOTROC) showed that a clinically significant PFS benefit with optimal surgery among patients with stage IC to IV disease was limited to patients with less advanced disease [25].
Adding values of lesional SUVs may imply the importance of tumor burden, and it may depend on the number of metastatic lesions without information of tumor volume. In this respect, we calculated the metabolic tumor volume (MTV) and performed analysis using the sum of MTVs. However, preoperative MTV was not an independent prognostic factor of recurrence in the current study (data not shown). Here, we hypothesized that the locus of the metastatic tumor burden would have prognostic importance.
One of the main pitfalls of PET imaging is the non-invasive visualization of diffuse peritoneal carcinomatosis, with the tumor spread through small implants on the peritoneal surface: the problem emanates from the reduced spatial resolution of PET imaging (5-6 mm) that makes it unable to visualize minute tumor implants, as in miliary carcinomatosis.
We recognize several limitations of this study. Most notably is that it was a retrospective study performed at a single institution with a relatively small number of patients (n=55). There may have been selection bias. Not all patients with EOC underwent preoperative PET/CT during the study period. The physician's attitude to PET/CT may have influenced the referral of patients in the retrospective study design. Hence, our findings may not be generalizable to all EOC patients, as only selected patients may have been referred to PET/CT scanning, and image acquisition and interpretation procedures will be different according to institutions. Additional standardized large prospective studies may be necessary to confirm the prognostic value of preoperative PET/CT in clinical practice. Secondly, we could not analyze the overall survival because there was only one case of disease-related death among the study population, and the study period was relatively short since PET/CT has only recently been introduced at our institution. We are preparing a prospective study to confirm the currently reported results, and eventually to determine if pretreatment PET/CT has predictive prognosis value.
Although this study has some limitations, it also demonstrates unique and significant findings, because to the best of our knowledge no study published to date has demonstrated the prognostic significance of metabolic burden in patients with EOC. The findings of the current study have important implications for the management of patients with EOC; patients with high SUVlocation ratio in preoperative PET/CT scan should be closely monitored after treatment, or consolidation treatment after previously-planned therapy may be seriously considered. In addition, targeting molecular therapeutics using tumor metabolism might be proposed and be a candidate theme of future research in the treatment of EOC.
In conclusion, preoperative SUVlocation ratio was a significant prognostic indicator for recurrence in patients with EOC, and may allow individualization of patient care. Further analysis with a larger patient population and longer follow-up is warranted for confirmation of the findings of this study.



 XML Download
XML Download