

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite tremendous improvements in treatment strategies against epithelial ovarian cancer, epithelial ovarian cancer is still the most lethal tumor among gynecologic malignancies, and is the fourth most common cause of cancer-related deaths among women worldwide.
Although ovarian cancer has not been traditionally considered to be responsive to immunotherapy, there is increasing evidence that indicates ovarian cancers are immunogenic. This evidence is derived from numerous clinical findings showing spontaneous antitumor immune responses [1-4], tumor immune evasion mechanisms [5-7], and clinical responses to immunotherapy [8-13] in patients with ovarian cancer, highlighting that immunotherapy may be applicable to treating ovarian cancer.
Although there have been successful reports of cancer immunotherapy in animal studies, clinical findings are disappointing with little improvement of survival outcome in patients. It has been reported that inefficient tumor rejection is not only the passive result of insufficient effector cells [14], but that tumors also actively fight back by utilizing immune-suppressive mechanisms that protect them from eradication [14,15].
CD73, also known as ecto-5'-nucleotidase (ecto-5'-NT) or 5'-nucleotidase (5'-NT), is a glycosyl-phosphatidylinositol-linked 70-kDa cell surface enzyme that is encoded by the NT5E gene. Normally, CD73 is expressed on endothelial cells and subsets of hematopoietic cells. CD73 was originally defined as a lymphocyte differentiation antigen. It likely acts as a cosignaling molecule on T lymphocytes, and is important as an adhesion molecule for lymphocyte binding to the endothelium [16,17]. CD73 catalyzes the dephosphorylation of adenosine monophosphate (AMP) and other nucleoside monophosphates [17]. Consequently, adenosine is accumulated in interstitial fluid from the dephosphorylation of AMP. Extracellular adenosine inhibits T lymphocyte activation and effector function by signaling primarily through A2a and A3 adenosine receptors on the surface of T cells. A2a adenosine receptor signaling has also been implicated in the inhibition of cytokine production and cytotoxic activity by natural killer cells [18]. CD73 is widely expressed on many tumor cell lines and is upregulated in cancerous tissues including those of the colon, lung, pancreas, and ovary. CD73 is also associated with drug resistance, tumor cells proliferation, tumor neovascularization, invasiveness, and metastasis of cancer cells [19,20]. These data suggest that CD73 expressed on tumor cells might function as the negative regulator of tumor control immunologically.
Considering the above-mentioned functions of CD73, patients with cancer cells expressing more CD73 are likely have poor survival outcome. However, only sparse information is available regarding the survival influence of CD73 expression on tumor cells in patients with malignancies. Therefore, the purpose of the current study was to evaluate survival outcome according to the expression status of CD73 in patients with epithelial ovarian cancer.
MATERIALS AND METHODS
1. Enrolled patients
We searched for patients with epithelial ovarian cancer who underwent staging operations with or without adjuvant chemotherapy in our department in an oncology database maintained at our department. Inclusion criteria were as follows: 1) patients with epithelial ovarian cancer (query term; serous, mucinous, clear, endometrioid, transitional, malignant Brenner); 2) patients who underwent primary therapy in our department; and 3) patients diagnosed between January 2000 and December 2010. This retrospective study was approved by the Institutional Review Board of Daegu Catholic University Medical Center.
Applying the inclusion criteria, a total of 167 patients with epithelial ovarian cancer were enrolled in the current study. For each patient, a retrospective review of medical records was conducted. The histologic slides of the surgically removed ovarian cancer tissues were reviewed again by 1 pathologist (HKO), who was blinded to the clinical variables of the patient.
2. Definitions of overall survival and disease-free survival
Overall survival (OS) was defined as the time from the date of diagnosis to death from epithelial ovarian cancer. Patients who survived beyond the time of analysis were censored at the time of their last follow-up date. Disease-free survival (DFS) was defined as the time from date of diagnosis to the recurrence of cancer in any sites.
3. Construction of tissue microarrays (TMA)
Representative paraffin tumor blocks were selected according to the primary evaluation of H&E stained slides of ovarian cancer before they were prepared for TMA. Two tumor tissue cores (1 mm in diameter) were taken from each of the donor ovarian cancer tissue blocks with a manual punch arrayer (Quick-Ray, Uni-Tech Science, Seoul, Korea). The cores were placed in a new recipient paraffin block that ultimately contained 59 to 91 tissue cores. Each array block contained both tumor and control tissue (lung, breast, and prostate cancer tissues and normal breast, colon, endometrium, ovary, and tonsil tissues) samples. Multiple sections (5 µm in thickness) were cut from the TMA blocks and then mounted onto microscope slides. The TMA H&E stained sections were reviewed under light microscopy to confirm the presence of representative tumor areas.
4. Immunohistochemical staining
Immunohistochemistry was conducted on 5 µm thick TMA tissue sections using the Bond Polymer Intense Detection System (Leica Microsystems, Mount Waverley, VIC, Australia) according to the manufacturer's instruction with minor modifications. Briefly, the 5-µm thick sections of formalin fixed and paraffin embedded TMA tissues were deparaffinized with Bond Dewax Solution (Leica Microsystems), and an antigen retrieval procedure was performed using Bond ER Solution (Leica Microsystems) for 30 minutes at 100℃. The endogenous peroxidase was quenched following 5-minute incubation with hydrogen peroxide. Sections were incubated for 15 minutes at ambient temperature with a mouse monoclonal anti-CD73 antibody (ab91086, 1:100; Abcam, Cambridge, MA, USA), a mouse monoclonal anti-FOX-P3 (ab20034, 1:50; Abcam), a mouse monoclonal anti-CD8 antibody (m7103, 1:200; DAKO, Glostrup, Denmark), and a mouse monoclonal anti-CD68 antibody (M0876, 1:200; DAKO), using a biotin-free polymeric horseradish peroxidase-linker antibody conjugate system in a Bond-Max automatic slide stainer (Leica Microsystems). Human tonsil (CD8, CD68, and FOX-P3), and lung carcinoma (CD73) tissues were used as positive controls.
5. Interpretation of immunohistochemical stain
CD73 expression levels were graded on a scale of 0 to 3 based on cytoplasmic and membrane staining intensity and the proportion of positive tumor cells by an expert pathologist who was blinded to the patient's clinical records. The staining was graded as 0 if no cancer cells were reactive, 1 if staining was weakly positive in <1/3 of cancer cells, 2 if staining was weakly positive in >2/3 of cancer cells, or strongly positive in >1/3 of cancer cells, and 3 if staining was weakly positive in most cancer cells, or strongly positive in >2/3 of cancer cells (Fig. 1). Immunohistochemical staining for CD73 in ovarian cancer tissue was classified as negative (grade 0) or positive (grade 1 to 3). FOX-P3 nuclear expression was counted as positive mononuclear cells in 3 high power fields (×400) in each tumor core. CD8 and CD68 cytoplasmic and membrane expression levels were graded on a scale of 0 to 3 based on the proportion of positive mononuclear cells infiltrated in the intratumoral and peritumoral stromal tissue. Arbitrary cutoff points at 1% (grade 0), 5% (grade 1), 25% (grade 2), and 50% (grade 3) for each positive cell per infiltrated immune cells were used.
6. Statistical analysis
Comparisons of variables between the groups were based on the chi-square test and independent t-test. The OS and DFS were estimated by the life-table method of Kaplan-Meier. Differences in survival rates were assessed by the log-rank test. The p-values were the result of two-sided tests and p<0.05 was considered statistically significant. Multivariate analysis was performed by Cox regression hazard model. Statistical analysis was done using SPSS ver. 13 (SPSS Inc., Chicago, IL, USA).
RESULTS
Characteristics of enrolled patients are shown in Table 1. Briefly, mean age was 50.3 years, and the mean of the largest tumor diameter obtained from the imaging study (ultrasonography, computed tomography or magnetic resonance imaging) was 11.6 cm. The number of patients in each FIGO stage was as follows; stage IA 39, IB 4, IC 18, IIA 2, IIB 9, IIC 13, IIIA 2, IIIB 9, IIIC 60, and IV 11. In terms of pathologic types, serous adenocarcinoma account for 43.7%, mucinous adenocarcinoma 24.0%, endometrioid adenocarcinoma 18.6%, clear cell carcinoma 12.6%, and transitional cell carcinoma 1.2%, respectively.
The expression status of CD73 in immunohistochemical staining is shown in Table 2. A total of 29.9% (n=50) patients showed negative expression, and the other patients (70.1%) showed positive expression (from grade 1 to grade 3). Survival analysis was conducted according to CD73 expression status. Because all patients with positive CD73 expression showed similar survival outcome (5-year OS estimation of grade 1, 72.5%; grade 2, 77.9%; and grade 3, 66.7%, respectively; p=0.760), the patients were grouped as CD73 positive and CD73 negative groups for further analysis.
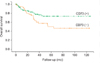
Contrary to our expectations, the CD73 positive group showed better prognosis compared to the CD73 negative group (5-year OS: CD73 positive group, 73.0%; CD73 negative group, 50.1%; p=0.023; 5-year DFS: CD73 positive group, 53.4%; CD73 negative group, 24.1%; p=0.021) (Fig. 2). Because there were more patients with mucinous adenocarcinoma in the CD73 positive group, we conducted a subanalysis for patients with non-mucinous adenocarcinoma. In a subgroup analysis for patients with non-mucinous epithelial ovarian cancer, although the difference did not reach to statistical significance, the CD73 positive group showed a tendency to have better overall survival than the CD73 negative group (5-year OS of the non-mucinous CD73 positive [n=81] and negative [n=46] group was 69.4% and 47.4%, respectively; p=0.052, Log rank test).
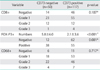
We compared the frequencies of CD73 overexpression (positive expression, from grade 1 to grade 3) according to clinicopathologic variables. CD73 was more frequently expressed in mucinous adenocarcinoma and clear cell carcinoma compared to serous or endometrioid adenocarcinoma. In addition, CD73 overexpressions were more frequently detected in patients with known good prognostic factors, i.e., low stage, well/moderate differentiation, negative peritoneal cytology, no lymphovascular involvement, and no macroscopic residual tumor after debulking surgery (Table 3).
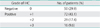
To evaluate the association of CD73 expression with immune cell deposition, we compared the differences in the degrees or numbers of immune cell depositions according to CD73 expression status. There were no differences in the depositions of cytotoxic T lymphocyte (CD8 positive cells) and monocyte/macrophage (CD68 positive cells) between the CD73 positive and CD73 negative group. However, there were significantly more Treg (regulatory T cell, FOX-P3 positive cells) in the CD73 negative group compared to the CD73 positive group (Table 4).
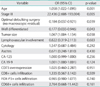
Multivariate analysis using Cox regression hazard model showed that age, stage, optimal debulking surgery, differentiation, and tumor size were independent prognostic factors, but CD73 overexpression was not (Table 5).
DISCUSSION
In this study, we observed that CD73 overexpression was more frequently observed in epithelial ovarian cancer patients with known good prognostic factors, including lower stage, well/moderate differentiation, negative peritoneal cytology, no lymphovascular involvement, and no macroscopic residual tumor. These resulted in patients showing CD73 overexpression had better survival outcome compared to those without CD73 expression. However, CD73 overexpression was not independent prognostic factor in multivariate analysis using Cox regression hazard model.
These findings were unexpected because CD73 expressed in tumor tissue has been reported to be detrimental to immunologic control of tumor in animal studies, and has been shown to be associated with tumor proliferation, metastasis, and invasion [19-21]. Previous studies showed that elevated levels of adenosine in solid tumors result in impaired killing of tumor cells by immune effector cells via multiple immune responses, such as inhibition of cytotoxic and helper T lymphocyte function, inhibition of the adhesion of cytotoxic T lymphocyte to cancer cells, and inhibition of natural killer cell function [18,19].
One possible explanation for the unexpected better outcome in the CD73 positive group is that overexpression of CD73 was more frequently observed in well/moderate differentiated carcinoma cells in this study. It is well known that a well differentiated cancer cell type is associated with lower stage. Lower stage results in more optimal surgery and better prognosis. Therefore, the result of our study means that favorable differentiation and stage have more influence on survival outcome than the adverse effect of CD73 per se on the host's local immune system.
Our findings are supported by those of Rackley et al. [22]. Rackley's group reported that CD73 (5'-nucleotidase) activity was lower in prostatic carcinomas than in benign prostatic hyperplasia [22]. They showed that the CD73 activity of prostatic carcinoma correlates well with the degree of histological differentiation; that is, the tissue extracts of poorly differentiated carcinomas contain lower levels of CD73 [22]. Our finding that negative expression of CD73 was associated with poorly differentiated carcinoma is in the same line with that of Rackley et al. [22]. Thus, it can be speculated that well differentiated cancer cells tend to produce more normal proteins including CD73 than poorly differentiated cancer cells.
Association of T cell infiltration in ovarian cancer tissues with survival outcome is a well known phenomenon [1-5,23]. In our study, however, there was no significant difference in CD8+ T cells infiltration levels between CD73 positive and negative patients. Instead, regulatory T cells were found less in CD73 positive patients showing better prognosis, as compared to CD73 negative patients. This data is consistent with the data of other groups in the aspect that patients having lower regulatory T cells infiltration have better prognosis [5]. However, considering that CD73 on tumor cells adversely affect the host immunologic response against tumor cells, our finding is unexpected. The reason for a lack of difference in CD8+ T-cell infiltration levels between the two patient groups is presently unknown. Similarly, we found no difference in the infiltration status of CD68+ cells (monocytes/macrophages) between the two patient groups.
In this study, CD73 overexpression was more frequently observed in epithelial ovarian cancer patients with known good prognostic factors, including well/moderate differentiation and lower stage. These findings show that differentiation status and stage have more influence on the survival outcome than the adverse effect of CD73 on immunologic environment. Because the effect of CD73 targeting therapy will be limited to patients with epithelial ovarian cancer with CD73 overexpression, CD73 targeting therapy will not be beneficial to patients with poorly differentiated ovarian carcinoma without CD73 expression. The limitations of the current study include the fact that it was a retrospective study, it had a limited number of enrolled patients, and it did not evaluate the functions of lymphocytes.



 XML Download
XML Download