

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ovarian cancer is one of the most severe gynecological malignancies known and is the fourth leading cause of cancer-related deaths in the United States [1], and has become the most lethal of all gynecological malignancies in Singapore women. Early stage disease has excellent prognosis but late stage disease has contributed to the high mortality rate of between 80% and 90% compared to early stage disease of between 10% and 30% [2]. Similar trends have been seen in Singapore women showing mortality of advanced stage at 77.1% and 20% in the early stage disease over a 5-year period [3]. The overall 5-year survival rate has not changed over the past thirty years despite the availability of new cytotoxic treatments [4] which showed dismal outcome, especially in advanced stage disease. Early detection remains the most important approach to improve long-term survival for ovarian cancer. Currently, CA-125 discovered nearly 30 years ago [5] remained the well-accepted serum biomarker for ovarian cancer but is neither specific nor sensitive enough for diagnosis [6-8]. It has clinical value for disease monitoring and has been used as an aid for early detection of relapse and for evaluation of response to treatment [9-11]. Prognostic indicators or biomarkers improve the accuracy of predicting patient outcomes, and until reliable screening or diagnostic strategies become available, they may contribute to the optimal tailored individual management of patients with ovarian cancer.
The current trend to focus on combined multiparametric analysis of different biomarkers to improve clinical outcomes and diagnosis will offer several advantages [12-15]. The group of serine proteases known as human tissue kallikreins (hK) has a rich source of cancer biomarkers and suited for multiparametric analysis. Human tissue kallikreins (KLK for gene, hK for protein) is a family of 15 members encoded by a group of genes tandemly localized on chromosome 19q13.3-4 [16]. It is highly expressed in sex organs such as the breast, ovary, prostate and testis. Emerging diagnostic markers notably hK6, hK10, and hK11 are highly expressed in the majority of ovarian cancer cases and especially in the advanced stage diseases [17-20]. The conventional CA-125 marker has shown negative values in 40% to 50% of early stage ovarian cancer and upregulated in benign tumors and other cancers [8,21]. However, tissue kallikrein proteins hK6 and hK10 together with osteopontin levels have been reported to be promising potential markers that might complement CA-125 in ovarian cancer [22]. It was suggested that the expression of hK6 may be an early event during ovarian cancer development and have potential use as biomarker for early detection of ovarian cancer [23] and prediction of progression-free survival [24]. In a small ovarian cancer cohort study, elevated levels of CA-125, hK6 and hK10 were seen. However, elevated serum hK6 levels was associated with mortality outcome within 12 months of diagnosis compared to those who survived over five years from epithelial ovarian cancer [3].
The objective of this collaborative study in South-East Asia from five Indonesian centers and one Vietnamese center in Ho Chi Minh City was to determine the value of ovarian cancer biomarkers hK6/hK10 and their association with CA-125 levels and age in patients with ovarian tumors for the prediction of epithelial ovarian cancer.
MATERIALS AND METHODS
1. Subjects
The study received approval from the National University of Singapore Institutional Review Board (NUS-IRB reference codes 05-025 and 06-067) and the respective ethics committee of various institutions involved in the study. Inclusion criteria were women with a pelvic mass detected by ultrasound at the hospital clinic and scheduled for operation. This was a prospective study and patients diagnosed with ovarian tumors were recruited to the study. Informed Consent was sought before they were allowed to take part in the study. Recruitment of subjects began in May 2005 in Medan, Indonesia and thereafter in various Indonesian centers; Denpasar (February 2006), Palembang (October 2006), Yogyakarta (December 2006), Jakarta (September 2007), and Ho Chi Minh City, Vietnam (April 2008) until August 2010. A total of 375 samples with confirmed patient information data were received; benign cysts 156, epithelial ovarian cancer 172 (stage I/II, n=72; stage III/IV n=100), germ cell cancer 36 and borderline 11. Administration of chemotherapy consisting of either cyclophosphamide, taxol and platinum drugs was recorded only for 26.2% (45/172) epithelial ovarian cancer patients. Most of the cancer patients were lost to follow-up and survival outcome analysis was not possible as most of them returned to their hometown soon after their diagnosis and surgery or after chemotherapy and did not returned for follow-up visits. Benign cyst cohorts were significantly younger with mean age of 38.3±1.2 years (95% CI, 35.9 to 40.8) compared to ovarian cancer patients with mean age of 45.5±1.0 years (95% CI, 43.5 to 47.5).
2. Blood collection
Blood sampling was performed in the morning before the scheduled operation. A clean venepuncture was performed together for hemostatic analysis, about 5 mL of plain blood was transferred in to clean plastic tubes. The blood tubes were then left at room temperature to clot for about 2 hours before they are centrifuged at 2,000 g for 15 minutes. The available sera was stored in aliquots and immediately kept at either -40℃ or -70℃ until dispatched to Singapore for storage at -80℃ and analysis.
3. Laboratory assays
CA-125 assay was performed by IMMULITE 1000 systems (Siemens, Los Angeles, CA, USA). Elisa assay for serum hK6 and hK10 was performed at the Pathology & Laboratory Medicine, Mount Sinai Hospital, Toronto, Canada, after consultation. It is a two-step sandwich immunoassay described earlier by Diamandis et al. [25].
4. Statistical analysis
All statistical analysis was performed using SPSS ver. 18.0 (SPSS Inc., Chicago, DE, USA). Group means were tested and compared by t-test. A p-value of less than 0.05 was considered statistically significant. Receiver operating characteristics (ROC) analysis were performed to determine the optimal cutoffs for age, CA-125, hK6 and hK10 levels. The sensitivity, specificity, positive predictive value (ppv) and negative predictive value (npv) for single and combination of markers were determined for the detection of ovarian cancer, early and advanced stage of disease.
RESULTS
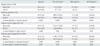
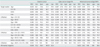
The types of benign cysts and epithelial ovarian cancer in the cohorts studied are shown in Table 1. The comparison of mean values of age, CA-125, hK6, and hK10 between benign cysts and epithelial ovarian cancer are shown in Table 2. Benign cyst cohorts from the Vietnamese center (n=44) and the Indonesian centers (n=112) showed no significant differences in the parameters studied. Hence, they were grouped together in the final analysis. Ovarian cancer cohorts were significantly older with a mean age of 45.5 years compared to 38.3 years in benign cyst cohorts and showed significant upregulation (p<0.001) of CA-125, hK6, and hK10 levels compared to benign cyst cohorts. In early stage ovarian cancer cases, significantly elevated levels of CA-125 (p=0.04), hK6 (p=0.03) in addition to older age (p=0.005) were observed compared to benign cyst cohorts. In addition, significant upregulation of CA-125 (p<0.001), hK6 (p=0.001), and hK10 (p=0.001) levels together with older age (p=0.002) were also seen in advanced stage diseases compared to benign cyst cohorts. When comparing early and advanced stage diseases, CA-125 (p=0.03) and hK6 (p=0.04) were significantly elevated in advanced stage disease with no significant differences in hK10 level and age. The variable scatter plots for the markers studied in benign cyst, early and advanced stage cancer are shown in Fig. 1. No significant differences in age, hK6 and hK10 levels between germ cell cancer (n=36) and benign cyst cohorts except CA-125 level which was significantly elevated (p=0.04) with mean value of 377.3±224.2 IU/mL (data not shown). The highest hK6 and hK10 levels were expressed by mucinous cancer (mean, 10.0±2.6 ng/mL and 3.3±1.2 ng/mL respectively), whilst in benign cyst cohorts, the endometroid type showed relatively elevated levels of hK6 (mean, 4.6±0.6 ng/mL) with hK10 mean levels of between 1.0 to 1.2 ng/mL seen for different benign types including endometroid cysts. Optimal cutoffs determined by ROC analysis for age, CA-125, hK6, and hK10 were 42 years, 93.0 IU/mL, 6.0 ng/mL, and 1.4 ng/mL, respectively and they were all above the mean levels of benign cyst cohorts (Table 2). The combination of either hK6 or hK10 with CA-125 showed potential as ovarian cancer prediction. The 3-combined markers of either age/CA-125/hK6 or CA-125/hK6/hK10 had 100% specificity and ppv with npv 54.1%/55.6% and sensitivity 18.8%/19.2% respectively for ovarian cancer prediction. The 4-combined markers age/CA-125/hK6/hK10 also showed 100% specificity and ppv with sensitivity 11.9%. When all 4 combined markers are negative, no advanced cancer is predicted with 100% specificity and ppv. The predictive values of various combinations of epithelial ovarian cancer markers are shown in Table 3.
DISCUSSION
Promising predictive tumor markers have been evaluated in patients with ovarian cancer. These combinations of markers showed promise to improve sensitivity and specificity, and in one study of four-marker panel which included CA-125, apolipoprotein A-1, transthyretin and transferrin, it was reported to improve sensitivity (96%), specificity (98%) for early stage ovarian cancer but has yet to be validated in clinical trials [26]. An earlier study using four-analyte test (leptin, prolactin, osteopontin, and insulin-like growth factor II) exhibited sensitivity 95%, ppv 95%, and npv 94% [27]. Proteases have emerged as important prognosticators in ovarian cancer [28] and the human tissue kallikrein family showed promise as biomarkers for ovarian cancer diagnosis, prognosis and monitoring [17,18,20]. Elevated serum or tissue levels of hKs have been individually implicated as diagnostic and prognostic factors in ovarian cancer [18,29 32]. In advanced stage disease, serous histological type and large residual tumor are known indicators for aggressiveness and poor outcome in ovarian cancer [30]. Proteases are widely believed to be involved in carcinogenesis and the concentration of proteases released by the primary tumor may reflect the ability of a tumor to spread [33,34]. Combined serum hK6 and hK10 can increase the diagnostic sensitivity of CA-125 in patients with early stage (I/II) ovarian cancer [29]. In the current study, the combination of hK6 and/or hK10 with CA-125 improved the specificity and ppv for the detection of ovarian cancer, despite the lower sensitivity.
In this study from South-East Asia, the ovarian cancer cohorts was significantly older with upregulated levels of CA-125, hK6, and hK10 than those observed in benign cyst cohorts. Early stage cancer showed older cohorts with significant upregulation of CA-125 and hK6 levels when compared with benign cyst cohorts. Only CA-125 and hK6 levels were further raised in advanced stage disease compared to early stage. The ovarian cancer cohorts from this study were younger (mean, 45.5 years) than reported for the incidence in postmenopausal women in the United States (mean, 60 years) and Scandinavia (mean, 61 years) [35,36]. Expression of the highest levels of hK6/hK10 in ovarian cancer were seen in mucinous cancer, contrary to the serous type reported [32]. In benign tumors, endometroid type expresses the highest hK6 levels whilst hK10 was not appreciable. In germ cell tumors, neither hK6 nor hK10 were upregulated except for raised CA-125 levels.
The proposed combination of biomarkers, including hK6, hK10, CA-125, and age, which cutoffs were determined by ROC analysis showed potential in improving the prediction of epithelial ovarian cancer in patients presenting with ovarian tumors. We analyzed various combination of the 4 markers for their ability to predict ovarian cancer, in early and late stage disease. Using this approach, the combination of 3 markers including age/CA-125/hK6 and hk6/hK10/CA-125 showed 100% specificity and ppv despite lower sensitivity, similar to the 4-marker combination of age/CA-125/hK6/hK10. No advanced cancer is predicted if the 4 combined markers are negative. The template proposed for predicting ovarian cancer may not meet the WHO criteria for screening tests which defines that high sensitivity and specificity are required during development of screening tests to detect early stage disease [37]. Screening tests must achieve at least 75% sensitivity and specificity of greater than 99.6% to achieve a positive predictive value of 10% for the detection of all stages of ovarian cancer [38]. Moreover, there may be limitations to this approach as full ultrasonography details are lacking but further study with the inclusion of ultrasonography can better enhance the potential value of these markers.
The analysis of combined markers may be a better choice than the use of CA-125 alone to predict ovarian cancer. Whilst the markers may be combined with CA-125 in improving the overall specificity of ovarian cancer detection, further investigation is needed to refine and evaluate the marker panels as a screening and detection modality [39]. The combination of multiple biomarkers and early screening modalities may be the key to obtain the most accurate forms of ovarian cancer detection. It is also important to identify screening techniques with low false positive rates and high positive predictive value so that negative surgical interventions can be minimized [39].
In conclusion, ovarian cancer cohorts from the region were older with upregulated levels of CA-125, hK6, and hK10. The combination of hK6 and hK10 with CA-125 and age demonstrated the potential for improved prediction of epithelial ovarian cancer, early and late stage disease in patients presenting with ovarian tumor.


 XML Download
XML Download