

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pseudomyxoma peritonei (PMP) is a rare, chronic relapsing disease in which cancer cells in the abdomen produce excessive mucous. Only a few pregnancies have been reported among patients with PMP, and there are limited data on the reproductive options available to affected women [1-6]. The course of pregnancy in patients with PMP is also not well documented. Advancements in fertility-sparing technologies and improved oncologic outcomes have led to increased interest in fertility preservation for young women with cancers that are scheduled to undergo surgery, chemotherapy and/or radiotherapy. Fertility preservation for women includes medical and surgical treatment and cryopreservation of embryos and oocytes, in vitro maturation and ovarian tissue cryopreservation. The decision of which procedure to recommend depends upon the primary malignancy, treatment protocol, age, and marital status of the patient.
This report describes a case of a young unmarried nullipara who underwent fertility preservation by means of in vitro fertilisation (IVF) with embryo cryopreservation prior to radical surgery and adjuvant chemotherapy for PMP. Thawed embryos were successfully transferred when she was disease-free.
CASE REPORT
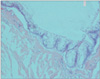
The patient was a 33-year-old unmarried nullipara whose family history was remarkable only for her brother having been diagnosed with testicular cancer. At the age of 28 years, she underwent explorative laparoscopy due to nonspecific abdominal pain, and a gelatinous tumor spread was detected. Biopsy specimens confirmed the diagnosis of disseminated peritoneal adenomucinosis (DPAM), which is a subtype of PMP (Fig. 1). These peritoneal lesions originated from perforated mucinous cystadenoma of the appendix. She was advised to undergo peritonectomy and bilateral oophorectomy. Prior to surgery, she was referred for consultation on fertility preservation options and decided to undergo the recommended IVF and embryo cryopreservation procedures. Twenty oocytes were retrieved and 18 embryos were fertilized with donor sperm and cryopreserved at the 2 pronuclear stage. The Institutional Ethical Committee approved the embryo cryopreservation procedure as well as the freezing protocol.
The PMP surgery was performed by a multidisciplinary team. Extended spread of the disease was found in the Douglas pouch, over the omentum, underneath the diaphragm, over the spleen with two large masses on both ovaries, a mass on the appendix and a number of lesions over the surface of the uterus. The parietal peritoneum was resected, and an omentectomy, appendectomy, splenectomy and bilateral adnexectomy were performed. Since it was possible to peel off the lesions that were located over the uterus, it was decided to leave the uterusintact in order to preserve future fertility. Postoperatively, the patient received heated intraperitoneal infusions of mitomycin C.
Eighteen month later, the disease relapsed as was evident by moderate elevation of carcinoembrionic antigen (CEA) and by intra abdominal fluid accumulation with multiple peritoneal lesions (by computed tomography). Explorative laparotomy showed numerous small lesions over the peritoneum, the left diaphragm and a lesion over the posterior wall the uterus. The patient underwent cytoreduction and peritonectomy followed by a 5-day intraperitoneal infusion of 5-fluorouracil (600 mg/m2/day) and remained disease-free for more than 7 years thereafter.
At the age of 37 years, she expressed her desire to become pregnant and, after consultation with the institutional oncologists, preparation of the endometrium was based on administration of 2 mg tid E2 valerate (Progynova; Schering Health Care Ltd., West Sussex, UK). Vaginal administration of micronized progesterone (200 mg tid, Utrogestan; Besins International Laboratories, Paris, France) was added to the drug regimen when endometrial thickness reached 8 mm. Three of the 9 surviving thawed embryos were transferred, and her hCG was positive 12 days later. It had doubled within 48 hours. At 21 weeks' gestation, she was diagnosed with deep vein thrombosis (DVT) and started on enoxaparin. It was difficult to anatomically identify the uterine cervix on ultrasonography (USG), since the urinary bladder appeared to be "smeared" all over the uterus, up to the fundus. During gestational week 28, she presented with left flank pain and gradual elevation of creatinine (up to 1.4 mL/DL). Single course of Betametasone (2 doses of 12 mg, IM-24 hours apart) was given for fetal lung maturation. An abdominal USG demonstrated mild bilateral hydronephrosis and there was no evidence of urine jets. It also showed that the urinary bladder covered the anterior part of the uterus. Doppler USG ruled out renal vein thrombosis. Cystoscopy revealed a much distorted bladder trigone and, although it was difficult to view the uretral openings, a pigtail (6 F/26 cm) was inserted into the left ureter after which the symptoms gradually resolved. At gestational week 30, our patient suffered from urosepsis. It was decided not to take out the pigtail since the creatinine levels (1.2 mL/DL) were steady. Under intravenous antibiotic treatment her condition was markedly improved. At gestational week 32, she again complained of left flank pain and was now experiencing difficulty in urinating. Her blood creatinine had sharply risen to 3.1 mL/DL, and the urology consultant suggested nephrostomy by angiography.
It was decided to deliver the fetus due to the deterioration of the patient's condition. A cesarean section was ruled out because of the distorted anatomy and fear of injuring the organs in proximity to the uterus. The patient received oxytocin to induce labor (bishop score, 7), and a healthy male neonate weighing 1,545 g, was delivered vaginally and transferred to the neonatal intensive care unit. The patient reported immediate relief of the flank pain and could urinate at will immediately after delivery. She received 2 infusions of packed cells due to postpartum hemorrhage. The rest of the postpartum course was uneventful, and her blood creatinine level returned to normal. She was put on warfarin, and she and her baby were discharged home. She was referred to an oncologist, hematologist and urologist for further follow-up.
DISCUSSION
PMP is a rare progressive malignant disease process within the peritoneum characterized by the production of copious amounts of mucinous fluid, resulting in a "jelly belly". The condition is fatal if left untreated [7]. PMP may be associated with benign or malignant lesions of the appendix or ovary and (rarely) pancreas, fallopian tubes and intestines. It preferentially affects women in the age range of 29 to 76 years, with a peak at 53 years [8]. Symptoms may include abdominal or pelvic pain and/or bloating, distension, digestive disorders, weight changes, increased girth and infertility [9]. The disease is sometimes incidentally discovered during surgery for other conditions or during a cesarean section [1]. The 5- and 10-year survival rates are 50% and 20%, respectively.
Low grade tumors of PMP are classified as DPAM and highgrade tumors are classified as peritoneal mucinous carcinomatosis (PMCA), with an intermediate group (IG) demonstrating a mixture of DPAM and PMCA. Survival was significantly higher in the low-grade (DPAM) as compared with the highgrade tumors (IG and PMCA) [10].
Aggressive surgical debulking, remains the primary treatment of PMP. Surgery may have to be repeated due to the recurrent nature of the disease. Postoperative adjuvant therapy includes intraperitoneal 5-fluorouracil, mitomycin-C and cisplatin.
A literature search using the terms "PMP", "pregnancy" and "infertility" revealed only a few case reports [1-6], probably due to the rarity of this disease (Table 1). Two of these cases were incidentally found [1,2]. Masakazui et al. [3] described a woman with acute abdomen secondary to small bowel obstruction at 34 weeks' gestation. Hales et al. [5] reported a case of secondary infertility attributed to PMP caused by ruptured mucocele of the appendix: resection of the tumor and visible mucinous ascites resulted in spontaneous conception. Narvekar et al.'s [6] PMP patient was successfully impregnated by egg donation, which was the method decided upon for her due to the presence of persistent multiloculated cysts in both ovaries and the absence of demonstrable normal ovarian tissue which made controlled ovarian hyperstimulation impossible.
Our patient desire to have a child had to be addressed. It is well known that the presence of pseudomucin in the peritoneum and the distorted tubo-ovarian relation secondary to the dense adhesions may impair fertility. Natural conception can occur but only rarely after surgical clearance and chemotherapy [4,5]. IVF may be an option when corrective surgery is precluded by dense adhesions. Narvekar et al. [6] reported that they were able to manage this problem by using IVF and donor eggs. In this case report we offered our patient emergency IVF and embryo cryopreservation before she underwent radical surgery and adjuvant chemotherapy.
To the best of our knowledge, this is the first case report of a patient with PMP, who conceived with IVF using embryos cryopreserved prior to definitive surgery and chemotherapy.
During pregnancy, complications related to PMP, like bowel obstruction, fistula formation may occur, with our patient we were dealing with DVT, elevated kidney and liver function tests, urosepsis and preterm delivery. Differential diagnosis included preeclampsia, renal vein thrombosis, recurrence of the primary disease and obstructive uropathy. Before the induction of labor, there was some debate over whether to perform a cesarean section or induce labor for a vaginal delivery. We recognize that it was fortunate that our patient delivered with no complications. Narvekar et al. [6] reported a PMP patient who underwent caesarean section after a failed induction. Her bladder turned out to be pulled up and adherent to the anterior uterine wall, and there was an inadvertent intraoperative injury to the bladder which had to be repaired following delivery.
This case report describes the successful outcome of fertility preservation measures that were taken prior to radical surgery and chemotherapy for PMP. Our patient is now 24 months post-delivery and both she and her son are doing well. She is being monitored by the specialists to whom she was referred.

 XML Download
XML Download