

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The significance of human papillomavirus (HPV) 18 genotype in treatment outcome is one of the most controversial issues regarding HPV-related human tumors [1-7]. In most of the studies regarding this subject, low frequency of HPV 18 infection (around 10% to 20%) often resulted in borderline or less than a statistically significant impact on prognosis [1,4,5,7]. Likewise, Kim et al. [7] showed a tendency for the HPV 18 genotype to be associated with poor disease-free survival (DFS) and with a trend for poor local control. However, the significance of HPV 18 was lost in multivariate analysis in that study.
Because a recent large-scale study showed that HPV 18 is a strong prognostic factor for relapse-free survival in patients with early-stage cervical cancer treated by surgery [4], the authors felt that it was important to clarify that the tumors with HPV 18 infection are also associated with poor outcome after radiotherapy. If such an association exists, it would be necessary to make efforts to develop a new treatment method in this subset of patients.
MATERIALS AND METHODS
1. Study population and treatment
This study was performed under the approval of our Institutional Review Board, and informed consent was obtained from all patients. The patients included 181 consecutive radiotherapy patients with International Federation of Gynecology and Obstetrics (FIGO) stage IIA-IVB cervical cancer treated between July 2003 and December 2008 at the National Cancer Center, Korea. Of 181 patients, 167 patients were included in our previous study [7]. Staging work-up included bimanual physical examination, posterior-anterior chest radiography, cystoscopy, and rectosigmoidoscopy in all patients. Magnetic resonance imaging of the pelvis±abdomen was obtained in 180 patients, and either positron emission tomography (PET) scan or PET/CT scan was obtained in 140 patients. Thirty-seven patients included in the previous institutional protocol undertook laparoscopic lymph node staging prior to radiotherapy.
Radiotherapy consisted of whole pelvic external beam radiotherapy (EBRT) and high-dose-rate (HDR) brachytherapy. Midline block was inserted at 36-45 Gy, giving a whole pelvic radiotherapy dose of 45-50.4 Gy. HDR brachytherapy was performed at the beginning of midline block with fractional doses of 4-5 Gy and 5-7 fractions twice a week. Median treatment duration was 58 days (interquartile range, 54 to 64). Most patients were treated with concomitant weekly cisplatin 40 mg/m2 during EBRT, except the 9 patients of stage IVB patients who received concurrent 5-fluorouracil/cisplatin chemotherapy with extended-field radiotherapy. Chemotherapy was not given at all in 19 (10.5%) patients because of their advanced age and expected poor compliance to concomitant chemoradiotherapy. After the conclusion of primary treatment, patients were followed up at 3-month intervals in the first 2 years, at 4-month intervals in the third year, and every 6 months thereafter. Two patients with tumors that showed negative HPV DNA in both HC2 and HPV genotyping were excluded from the study due to the lack of HPV genotype information. Patients with multiple infections including the HPV 18 were grouped as HPV 18 infection.
2. Extraction and amplification of HPV DNA and HPV genotyping by LiPA
Genomic DNA was extracted from paraffin-embedded tissue sections or frozen tissues using the QIAamp DNA mini kit (Qiagen, Hilden, Germany). The SPF10 polymerase chain reaction was performed and the amplimers were subsequently analyzed by reverse hybridization on the HPV reverse hybridization line probe assay (INNO-LiPA HPV Genotyping CE [LiPA]; Innogenetics N.V., Gent, Belgium) under the manufacturer's instructions. LiPA permits the specific detection of 16 HPV genotypes, including 14 high-risk HPV (16, 18, 31, 33, 40, 45, 51, 53, 54, 58, 59, 66, 68, 70) and 2 low-risk HPV (HPV 6, 11).
3. Statistical analyses
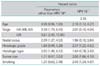
Demographic and clinical characteristics are presented as counts and percentages for categorical variables; median and range are supplied for continuous variables. The distributional differences between groups were assessed using the Pearson chi-square test or Fisher's exact test. As measures of prognostic outcome, DFS and local recurrence-free survival were considered. The multivariate Cox proportional hazards model was employed to adjust the effects of other potential confounding factors such as age, HPV type 18, stage group, nodal status, tumor size, histologic grade, histologic type, and smoking status. The final multivariate Cox model was chosen based on the combination of a stepwise procedure and the hierarchical selection method, as well as consideration of the clinical or biological importance of the variables in the model. A bivariate Cox regression was performed for HPV 18 with other parameters to detect the factor(s) which might have influenced the prognostic significance of HPV 18. All statistical analyses were performed using SAS ver. 9.1 (SAS Inc., Cary, NC, USA). Kaplan-Meier curves were generated using STATA ver. 10 (Stata Co., College Station, TX, USA). All reported p-values are two-sided.
RESULTS
1. Treatment outcomes and clinical variables
From the beginning of the observed study period until the time of analysis, 54 patients had disease progression, including 40 distant metastases and 18 local recurrences. Five patients developed both local and distant recurrences. The patients were followed up for a median period of 33 months (range, 2 to 72 months). The median follow-up for the patients without recurrence was 42 months (range, 6 to 72 months).
HPV 18 was detected in 20 of the 181 patients (11%) as a single (11) or multiple infections (9). Adenocarcinoma (AD) histology was 17 with 11 AD and 6 adenosquamous carcinoma (ASC). Patients' characteristics are shown in Table 1 in relation to HPV 18.
2. Univariate and multivariate analyses of radiotherapy outcome
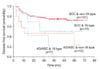
Both HPV 18 and AD/ASC histology were associated with poor DFS in univariate analysis, with hazard ratios of 2.37 and 3.56, respectively (Fig. 1, Table 2). Other prognostic parameters for DFS included HPV 18, advanced stages, presence of nodal metastasis, poorly-differentiated histologic grade, and tumor size larger than 4 cm. In multivariate analysis, advanced stages and AD/ASC histologic type were significantly related to DFS (Table 2).
3. HPV 18 and associated clinicopathologic characteristics
HPV 18 was also associated with larger tumor size, positive nodal status, and also marginally associated with poor histologic differentiation (χ2 test, p=0.04, 0.05, 0.06, respectively). Most prominently, tumors with HPV 18 type were associated with AD/ASC (92% vs. 8% in squamous cell carcinoma [SCC], 59% vs. 41% in AD/ASC for non-18 vs. 18 type, χ2 test, p=0.001). When bivariate Cox regression analysis was performed, the hazard ratio of each parameter remained the same regardless of HPV 18 genotype except for the histologic type for which the hazard ratio has significantly decreased from 2.38 to 1.64 (Table 3). When a combinational group of HPV 18 vs. non-HPV 18, and AD/ASC vs. SCC histology was made and compared, univariate Cox regression analysis revealed that the hazard ratio was increased to 2.1 (95% confidence interval [CI], 0.87 to 4.86; p=0.10), 3.67 (95% CI, 1.54 to 8.74; p=0.003), and 4.05 (95% CI, 1.58 to 10.33; p=0.003), for SCC/HPV 18, AD/ASC/non-HPV 18, and AD/ASC/HPV 18, respectively (Fig. 2) compared to the risk of SCC/non-HPV 18 group. Although statistical significance was not shown, there was a strong tendency for patients with SCC/HPV 18 infection to do worse than SCC/HPV non-18 infection. Five of seven (71.4%) in 18 type in AD/ASC and 6/10 (60%) in non-18 type in AD/ASC relapsed. Four out of 5 ASC showed HPV 18 infection and all of them failed locally and distantly.
DISCUSSION
In the present analysis, we tried to show the effect of HPV 18 on the outcome of patients with cervical cancer treated with concomitant radiochemotherapy. From the results of our study, it is hard to conclude that HPV 18 is a strong prognosticator on its own, because prognostic significance remains stronger for tumor histology than HPV genotype in multivariate analysis. Our bivariate analysis showed that the effect of HPV 18 on the inferior post-radiotherapy survival was negatively influenced by the relationship between HPV 18 and AD/ASC histology. However, the authors were not able to clearly show the interaction of HPV 18 and AD/ASC histology because the number of patients with AD/ASC tumors was only 17, and also the prognosis of patients with AD/ASC was poor on its own in the absence of HPV 18 infection. The effect of HPV 18 is only supported by the poorer survival which was observed in SCC/HPV 18 tumors compared to the SCC/non-HPV 18 tumors. In our study, the poor prognosis of AD/ASC tumors is mainly contributed by the poor prognosis of ASC tumors. There were 5 patients with ASC tumors and all of the patients failed locally or in distant sites; one patient had non-HPV 18 type and 4 tumors had HPV 18 type. For AD tumors, there was 1 failure in 3 HPV 18 types; however, there were also 5 failures in 9 non-HPV 18 types, making the conclusion that the poor prognosis of AD/ASC tumors is entirely due to the high proportion of HPV 18. The finding that 4 out of 5 cases of ASC showed HPV 18 infection is worth noting because many other authors reported that ASC histology is closely associated with HPV 18 infection. Fujiwara et al. [2] reported 11 patients with ASC who all showed HPV 18 infection in their tumors. HPV 18 was frequently associated with AD/ASC in our study and also in other studies [1,8-15].
We suggest the following common patient characteristics which can be observed in both HPV 18 and AD/ASC tumors. Firstly, median age of the patients is younger in patients with AD/ASC than in patients with SCC tumors [7,16-18], and also in patients with HPV 18 tumors than with non-HPV 18 tumors [5,19], which may indicate shorter period of carcinogenesis. Secondly, viral load is significantly lower in AD/ASC and HPV 18 tumors compared with SCC and non-HPV 18, respectively. In AD/ASC tumors, HPV detection rate ranges from 0-95% and 33.3-100% respectively and is frequently found to be lower than that of SCC [20]. It is not uncommon to find no detectable HPV DNA in AD/ASC [21-24]. The lower viral load of AD/ASC was also shown in our previous study and in other studies [7,20, 21]. It is also known that HPV 18 shows significantly low viral copy number in many studies [23]. Thirdly, AD of the cervix is increasing in incidence worldwide especially in developed countries [24,25]. According to a recent report, HPV16 cervical tumors are decreasing in incidence while those with HPV 18 do not [26]. All of these common clinical characteristics suggest a distinct biology of the two minor but important types of cervical tumors for which mechanisms of carcinogenesis needs to be explicated. Our analysis suggests that there are overlapping cancer biology between AD/ASC and HPV 18. In HPV 18 cervical cancer, earlier integration of the viral genome compared with other types is considered to occur during carcinogenesis, which in turn causes greater chromosomal instability, higher growth rates, and rapid progression of disease [16]. These biological characteristics are likely to cause radioresistance, chemoresistance, and finally poor prognosis which is supported by many preceding reports [27-38]. Further investigation is necessary to reveal the host factors lying behind our observation, along with the possible viral factors.



 XML Download
XML Download