

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endometrial cancer is the most common disease among gynecological cancers and is one of the main health concerns worldwide.1,2 In the United States alone, 41,200 women develop endometrial cancer, and about 7,350 women die from this disease annually.2 According to the Annual Report of Gynecologic Cancer Registry Program in Korea, the incidence of endometrial cancer in Korean women is recently increasing.1 Endometrial cancer may occur de novo, but can also arise within preexisting premalignant lesions exhibiting advanced degrees of hyperplasia.3 In 1994, according to the WHO classification, simple and complex types of hyperplasia are further subdivided into those with typical or atypical architecture.4 This is the most important distinction from the stand point of clinical management, because the risk of malignant transformation of hyperplasia to invasive carcinoma increases according to the classification of hyperplasia from 2 to 23% in premalignant lesions exhibiting without atypia to with atypia, respectively.5 The progression of a lesion from a premalignant state to endometrial cancer is believed to be the outcome of a series of metagenesis driven by various risk factors.3 The identification of specific intracellular events in carcinogenesis is a necessary prerequisite to the identification of therapeutics that target and interrupt specific steps in the progression of cancer.6
Previous studies have suggested a correlation between the expression of syndecan-1 and the development of cancer characteristics in the human endometrium.7 However, it is not yet clear whether syndecan-1 is closely correlated with the onset of tumorigenesis or if it plays a role as a positive predictive marker in cancer development. For these reasons, we sought to determine if quantitative analysis of syndecan-1 correlated with the histological classification of endometrial hyperplasia by evaluating syndecan-1 expression in endometrial hyperplasia and stage I, grade I cancer tissues by determining the percentage of positively stained cells to yield a quantitative value for syndecan-1 expression. Our results suggest the role of syndecan-1 as a predictive factor of progression from hyperplasia to endometrial cancer.
MATERIALS AND METHODS
1. Patients and tissue samples
Tissue samples were obtained from the paraffin-embedded endometrium of study 101 patients who underwent endometrial curettage and/or hysterectomy and were followed up at the Department of Obstetrics and Gynecology of Ajou University Hospital, Suwon, Korea between 1995 and 2007. The patient population consisted of individuals including endometrial hyperplasia (N=60). Endometrial data obtained were classified into five groups: normal endometrium (NE, N=10) as the control group, simple hyperplasia (SH, N=20), complex hyperplasia without atypia (CH, N=20), complex hyperplasia with atypia or atypical hyperplasia (AH, N=20), and endometrial cancer (EC, N=31) with grade 1 differentiation. NE was obtained from patients with intramural or subserosal myomas showing grossly and microscopically intact endometrium. Specimen was obtained from representative endometrial pathologies: hysterectomized endometrium (N=63) or endometrial curettage (N=38).
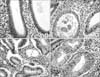
We performed a quantitative analysis of syndecan-1 expression employing a scoring method of the immunohistochemical staining frequency. Histopathologic classification of endometrial hyperplasia was based on the "International Society of Gynecological Pathologists" criteria. The histological grades according to the International Federation of Gynecology and Obstetrics (FIGO) staging classification were as follows: 31 patients in this study were grade 1. Surgical staging was reviewed based on the FIGO staging system and all of the endometrial cancer patients were stage I disease. Endometrial hyperplasia specimens were further subdivided by the presence of atypia and degree of differentiation. In all cases, atypical cells were identified on the original H&E sections (Fig. 1). Follow-up for all patients who had endometrial hyperplasia in the endometrial curettage specimen, as evidenced by staining with syndecan-1, was obtained when possible. We retrospectively reviewed patient charts to identify patient's demographic factors.
2. Immunohistochemical study
Serial paraffin sections were cut to 4 µm in thickness for immunohistochemical study of syndecan-1 expression in endometrial hyperplasia and endometrial cancer cells. Paraffin-embedded sections from clinical endometrial tissue samples were subjected to immunostaining for syndecan-1 using anti human syndecan-1 mouse B-B4 monoclonal antibody and DAB visualization, as described in the manufacturer's manual. In brief, after deparaffination and treatment of 3% H2O2 for 5 min, the tissue samples were blocked with a 10% serum in the blocking solution of the Histostain®-Plus Bulk Kit (Biocompare, San Francisco, CA, USA) for 1 hr and incubated overnight at 4℃ with anti syndecan-1 mouse monoclonal (B-B4 clone) antibodies at 1/400 dilution in the antibody diluent. For either tissue samples, DAB color reaction was performed with the Histostain®-Plus Bulk Kit before being examined under an Olympus microscope D50 (Olympus, Tokyo, Japan) and photographed using an AxioCam MRc5 camera (Carl Zeiss AG, Oberkochen, Germany). Then each stained section was counterstained with Mayer's hematoxylin. Also, the sections from the same tissues were stained with Mayer's hematoxylin and eosin for histological classification.
3. Staining evaluation
The level of syndecan-1 immunoreactivity in endometrial cells was expressed by scoring the percentage of syndecan-1 positive cells into four groups: 0, negative of cells stained; 1, <33% of cells stained; 2, 33 to 66% of cells stained; and 3, >66% of the cells stained.7 Microscopic analyses were evaluated independently by one pathologist (HJH) with no prior knowledge of the clinical data.
4. Statistical analysis
Distribution of the patients' characteristics was presented as mean (SD) for continuous variables, and frequency (%) for categorical variables including immunohistochemical staining. Fisher's exact test was used to determine the correlation between the two categorical variables. The Mann-Whitney U-test or Kruskall-Wallis test was used to compare the mean or median values between the two or more groups. A p-value <0.05 was considered statistically significant.
RESULTS
1. Patient characteristics
The mean age of included subjects at the time of diagnosis was 44 years (range, 21 to 71 years). There were no significant differences in age, gravidity, parity, body weight, menopausal status, diabetes status, and hormone replacement therapy status between the study groups. Demographic data of the patients are summarized in Table 1.
2. Expression of syndecan-1
The immunostaining of syndecan-1 in the control, endometrial hyperplasias and endometrial cancer tissues are shown in Fig. 2. The mean score of syndecan-1 immunoreactivity was 1, 0.6, 1.9, 2.6, and 2.2 in NE, SH, CH, AH, and EC, respectively (Fig. 3). The mean rank score of staining according to classification of endometrial hyperplasia is shown in Table 2. In other words, the mean ranks of expression scores based on the frequency of syndecan-1 staining were 31.6, 20.5, 52.9, 72.1, and 62.1 with NE, SH, CH, AH, and EC, respectively (Table 2). The differences were statistically significant (p<0.001).
In the subgroup analysis, syndecan-1 expression was significantly greater in CH (N=20, p<0.001) or AH (N=20, p<0.001) than SH (N=20). Syndecan-1 expression was significantly greater in AH compared to CH (p=0.028). Syndecan-1 expression was significantly greater in CH (p=0.042), AH (p<0.001), or EC (p=0.002) compared to NE. However, these differences in expression of syndecan-1 were not identified between SH and NE (p=0.248). Also, no significant difference was observed in syndecan-1 expression between AH and EC (p=0.085).
DISCUSSION
A number of immunohistochemical studies have demonstrated the aberrant expression or immunoreactivity of syndecan-1 in many malignancies, as well as a correlation of syndecan-1 expression with neoplastic progression, and inverse significance has been found in different tumors. For example, the expression of syndecan-1 in carcinomas of the head and neck regions,8 esophagus,9 larynx,10 liver,11 lung,12 colon,13 and uterine cervix14 was related to low clinical stage, favorable outcome, and better differentiation, whereas inverse results are noted in malignancies of the nasopharynx,15 breast,16 prostate,17 and thyroid.18
In endometrial cancer, there have been recent histological studies on endometrial tissues suggesting that the expression of syndecan-1 is closely correlated with the gain of carcinogenesis in the human endometrium.7
Syndecan belongs to the heparan sulfate proteoglycan family found as components of cell surface and take part in cell-cell interaction, cell-matrix adhesion, and growth factor signaling.19 Thereby, syndecan is known to regulate cell differentiation, proliferation, migration, and homeostasis.20-22 It has been reported that syndecan-1 may be a critical molecule in maintaining viability signals in endometrial cancer.7
Because syndecan-1 expression has a strong association with endometrial cancer,7 this study examined the expression of syndecan-1 in endometrial hyperplasia specimens by immunohistochemical stain which quantitavely analyzed syndecan-1.
Also, syndecan-1 expression was evaluated for significance according to the histologic types of endometrial hyperplasia, because the risk of endometrial hyperplasia progressing to carcinoma is related to the presence and severity of cytologic atypia.23,24 Kurman et al.4 found that progression to carcinoma occurred in 1% of patients with SH, 3% of patients with CH, 8% of patients with atypical SH, and 29% of patients with AH. As the above results indicate, there was significant difference in syndecan-1 expression according to the histologic classification of endometrial hyperplasia. Syndecan-1 expression was significantly greater in AH than SH or CH. Our results therefore further suggest that syndecan-1 expression is positively correlated with the risk of progression of endometrial hyperplasia to endometrial cancer. Thus, syndecan-1 immunoreactivity in endometrial hyperplasia appears to be a useful indicator of high risk for development of endometrial cancer.
Small sample size was a study limitation. Additional possible limitations of this study were sample selection and other confounders because of retrospective sample selection. We made an effort to minimize these limitations as much as possible.
Future studies will determine whether the extent of syndecan-1 expression in endometrial cancer correlates with prognosis. Also, there is a need for a prospective study for syndecan-1 as a reliable biomarker of aggressiveness in endometrial hyperplasia. Our findings lend support to a suggestion that the risk of endometrial hyperplasia progressing to carcinoma is related to the presence and severity of cytologic atypia. In addition, the current findings, which revealed that aberrant syndecan-1 expression is a property of both complex atypical hyperplasia and invasive carcinoma of the endometrium, raise the possibility that some or all foci diagnosed as complex atypical hyperplasia in fact may be endometrial adenocarcinoma in situ. Thus, syndecan-1 may be used as a diagnostic indicator of progression to endometrial cancer.




 XML Download
XML Download