

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rhabdomyosarcoma (RMS) is a malignant tumor which arises from embryonic muscle cells. It is the most common soft tissue sarcoma in childhood and young adulthood, and accounts for 4 to 6% of all malignancies in this age group.1 This tumor presents as a submucosal lesion giving the typical "grape-like" appearance and is usually seen in female infants and young children.2
Sarcoma botryoides is usually reported as a vaginal tumor in the female reproductive tract of infants.3 However, it also occurs rarely in the cervix or uterine fundus.4 An important matter is a higher level of survival and better prognosis of vaginal lesions. The survival rate of vaginal and cervical lesions have been reported to be of 96% and 60%, respectively.5
To our knowledge up to now, only one similar case of rhabdomyosarcoma in two sisters has been reported in the literature.6 Here, we report a case of sarcoma botryoides presenting as a cervical polyp in a 14-year-old girl and discuss its pathologic findings.
CASE REPORT
A 14-year-old girl presented with abnormal vaginal bleeding three months ago. Gynecologic examination revealed a cervical polyp protruding through the vagina and smooth parametria with no evidence of vaginal extension. Biopsy of the lesion was performed and histology examination was consistent with embryonal heterologous rhabdomyosarcoma. The patient underwent work-up for metastasis which was negative for any metastases. She underwent a type III radical hysterectomy and bilateral pelvic and paraaortic lymphadenectomy. Post-operatively, there was no evidence of gross remaining pathology. The final pathology showed lymph nodes and surgical margins free of disease. Histological examination of the specimen removed during surgery revealed a stage IA polypoid embryonal heterologous rhabdomyosarcoma. No adjuvant chemotherapy or radiotherapy was applied. Until the last follow-up 11 months following surgery, the patient remained disease-free and no local or remote metastasis has been documented.
1. Pathological findings
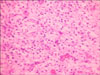
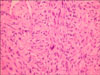
The specimen was composed of multiple polypoid soft tissue fragments up to 3.5 cm in dimension. Underlying a non-keratinizing squamous epithelium was an edematous stroma with plump stromal cells and moderate mitotic activity. A cambium layer was not clearly identified, but some of the stromal cells showed dense eosinophilic cytoplasm without apparent cross-striations (Figs. 1 and 2).
Familial history of the current patient revealed that her sister expired three years ago with the same diagnosis in another medical center. She was 17 years old at the time of the diagnosis. At first, she had undergone conservative surgery. Three months later radical hysterectomy and wide local excision of the cervical tumor was performed due to recurrence of the tumor. After the second surgery the patient developed several metastases which ended in the death of the patient. The histological examination of the polyp specimen also showed to be a rhabdomyosarcoma.
DISCUSSION
The emphasis of this report is on the probability of the role of genetic factors in sarcoma botryoides of the uterine cervix. Sarcoma botryoides in the cervix is rare, and most of the present knowledge is based on case reports. The largest series of sarcoma botryoides of the uterine cervix consisted of 13 patients.7 There are reports regarding various presentations and medical or surgical treatments used for these patients. However, it seems that reports with respect to cytogenetic studies and possibility of genetic factors contributing to both the formation and prognosis of this malignant tumor have not been studied extensively yet.
The botryoides subtype of embryonal RMS accounts for about 10% of all RMS cases and arises under the mucosal surface of body orifices such as the vagina, bladder and cervix. Although sarcoma botryoides of the cervix has been reported in females as young as five months of age, it tends to occur predominantly in older ages (i.e., children and young adults), than those which occur in the vagina. The tumors of the sisters described here were diagnosed in the second decade of their life. Vaginal bleeding which is the most common presentation was reported in our case as well. Most patients present with vaginal bleeding or a sensation of a mass in the introitus.5
The histological findings of sarcoma botryoides of the uterine cervix are similar to the ones which occur in other organs. These findings consist of rhabdomyoblasts of varying differentiation dispersed within a loose, myxoid stroma. A distinct "cambium layer" beneath the epithelium is characteristic of sarcoma botryoides.8 Several other lesions enter into the pathologic differential diagnosis, including adenosarcoma, edematous cervical mesodermal polyps (pseudosarcoma botryoides), rhabdomyoma, and other tumors.9 Adenosarcomas can also be found in young women but histologically can be distinguished from sarcoma botryoides by their fibrous stroma and leaf-like pattern of glands.7
The major surgical treatment for rhabdomyosarcoma which was performed in our patient consisted of complete resection of the primary tumor with a surrounding "margin" of normal tissue. Wide and complete resection of the primary tumor is less applicable to patients known to have metastatic disease at the initial operation.10 Daya and Scully7 reported that three of the 13 patients treated with fertility-sparing surgery (polypectomy or trachelecectomy) followed by chemotherapy had comparable results to those treated with more radical surgery with or without chemotherapy. This group suggested that, in contrast to sarcoma botryoides occurring in the vagina, cervical sarcoma botryoides has a favorable outlook. In the current patient, due to the familial history of the patient whose sister showed recurrence after primary conservative surgery, we decided to perform hysterectomy first.
The prognosis of sarcoma botryoides of the cervix is more satisfactory than other rhabdomyosarcomas of the genital system. The prognosis becomes better especially when the tumor arises in a single polypoid lesion and is completely removed during surgery.9 There are some prognostic factors defined for this tumor. Te majority of RMS cases occur sporadically and no predisposing factor is recognized for them. The Li-Fraumeni syndrome leads to a family cancer susceptibility syndrome which is documented by clustering of soft tissue malignancies (including sarcomas) to be caused by a heterozygous germ line p53 mutation.10 Unfortunately, none of the current patients had genetic consultation and therefore investigation of germline p53 mutation was not performed.
It is likely that a genetic component contributes to the development of sarcoma botryoides of the uterine cervix. In the previous report,6 cryptogenic studies for trisomy 13 and 18 were negative. However, deletion of the short arm of chromosome 1 and trisomies 13 and 18 in RMS of the cervix has been reported only in one study.8
A limitation encountered in this report was the lack of appropriate cytogenetic studies to detect any probable genetic factor. It is recommended that in the future, in cases of sarcoma botryoides of the female genital system, a complete study of genetic factors be done to detect any predisposing genetic agent. It is possible to achieve a satisfactory outcome in a short-term period with radical hysterectomy.
 XML Download
XML Download