

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer is the most prevalent gynecological malignancy in many developing countries.1 Surgery is the most effective therapeutic method in patients with invasive cancer confined to the cervix. The 5-year survival rate after surgery for patients with stage IB1 disease exceeds 90%, but is only 60-70% in patients with tumors >4 cm in size.2-4 Neoadjuvant chemotherapy has been administered to patients with locally advanced cervical cancer to improve outcome.5,6 Among the main advantages of neoadjuvant chemotherapy are the potential elimination of micrometastases, shrinkage of the primary tumor to achieve radical operability and the surgical down-staging of patients.7,8 Despite its high response rates,6,7,9-12 neoadjuvant chemotherapy for cervical cancer still remains controversial. While an Italian trial and a meta-analysis has demonstrated that neoadjuvant cisplatin-based chemotherapy followed by radical surgery affords survival benefits in patients with stage IB2-IIB cervical cancer,13,14 a recent phase III GOG trial failed to demonstrate any survival benefit.15 The discrepancies in these results may be due to a variety of clinical and biological factors, and the use of different chemotherapeutic regimens based on cisplatin.15-18 Several new drug regimens may have more activity in cervical cancer. We therefore tested the efficacy of paclitaxel plus platinum neoadjuvant chemotherapy in patients with stage IB2 to IIA cervical cancer of size >4 cm, as evaluated by MRI, on pathologic prognostic factor and long-term survival.
MATERIALS AND METHODS
All patients with stage IB2 or IIA cervical cancers with tumor size >4 cm on MRI treated with paclitaxel plus platinum between November 1, 1999 and September 30, 2007 were retrospectively reviewed. All patients had primary, previously untreated, histologically confirmed cervical cancer. Patients treated with other chemotherapy regimens were excluded. The patients with para-aortic lymph node metastasis or simultaneous other malignancies after primary surgery were also excluded. During the same period, the control group consisted of patients with tumor size >4 cm who underwent radical surgery alone, which was defined as the primary surgery (PS) group. Clinical staging procedures including pelvic examination, chest X-ray, cystoscopy, rectosigmoidoscopy, and intravenous pyelogram were performed in all patients. The patients underwent MRI to evaluate tumor size during the initial diagnostic procedure and just before surgery after 2 cycles of neadjuvant chemotherapy.
Neoadjuvant chemotherapy consisted of 2 cycles of intravenous paclitaxel 135 mg/m2 and cisplatin 75 mg/m2 or carboplatin AUC 5 3-week intervals interval. All patients underwent type III radical hysterectomy with systematic pelvic lymphadenectomy plus, if indicated, para-aortic lymphadenectomy, within 3 weeks of completion of the second chemotherapy cycle. Postoperative concurrent chemoradiation or radiotherapy alone was administered to high risk patients, defined as those with at least one major risk factor, including positive nodes, parametrial involvement and positive surgical margin, or two or more minor risk factors, including tumor size, depth of invasion and lymph-vascular space invasion (LVSI).
Tumor response was evaluated for tumor size measured by MRI at the initial diagnostic procedure and just before surgery after neadjuvant chemotherapy according to the Response Evaluation Criteria In Solid Tumors (RECIST).19 Only 42 patients who took pre- and post-chemotherapy MRI were assessed for tumor response. Complete response (CR) was defined as the complete disappearance of the tumor in the cervix, partial response (PR) as a ≥30% decrease of longest diameter (LD), progressive disease (PD) as a ≥20% increase of LD, and stable disease (SD) as a decrease or increase less than PR or PD. Patients who achieved CR or PR were defined as responders, whereas those who achieved PD or SD were defined as non-responders.
SPSS ver. 12.0 was used for statistical analysis. Categorical variables were compared using the Chi-square and Fisher's exact tests. Mean, median, and standard deviations were calculated for continuous variables, which were compared using the t test. Survival time was calculated from the date of the neoadjuvant chemotherapy was started. The survival rate was calculated by the Kaplan-Meier method and compared using the log-rank test. Statistical significance was defined as p<0.05.
RESULTS
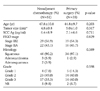
In this study, 51 patients received neoadjuvant chemotherapy (NAC) followed by radical hysterectomy and 35 underwent immediate radical hysterectomy. The two groups were similar in age at diagnosis, tumor size, level of squamous cell carcinoma (SCC) Ag, FIGO stage, and histological type and grade (Table 1).
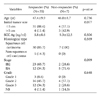
There were no life-threatening complications following chemotherapy. All patients successfully underwent radical hysterectomy and complete nodal dissection. After NAC, CR was observed in 3 of 42 (7.1%) patients, PR in 32 (76.2%) patients, and SD in 7 (16.7%) patients, making the overall response rate after NAC 83.3% (35/42). There were no significant differences in age, level of SCC Ag, and histological type and grade between responders and non-responders (Table 2). The patients with larger than 5 cm sized tumor or FIGO stage IIA showed poorer response, but there were no significant differences (p=0.077, p=0.099, respectively).
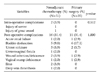
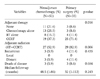
When we compared operative and pathologic data after radical hysterectomy in the two groups, we found no significant differences in operating time, estimated blood loss and the number of lymph nodes (Table 3). More patients in NAC group required blood transfusions and the postoperative change in hemoglobin was significantly lower (p=0.009). Nodal metastasis were observed in 35.3% (18/51) of the patients in NAC group, compared with 48.6% (17/35) in the primary surgery (PS) group; LVSI was observed in 43.1% and 57.2%, respectively, and parametrial involvement in 29.4% and 28.6%, respectively. However, tumor size was much smaller and cervical invasion was more superficial in NAC group. Despite that laparoscopic radical hysterectomy was mainly performed in the NAC group (23.5% vs. 2.9%, p=0.012), there were similar complication rates between the two groups (Table 4). Postoperative adjuvant therapy was administered to 40 patients (78.4%) of the NAC group and to 32 (91.4%) of PS group (p=0.142). Fewer patients treated with NAC received adjuvant radiotherapy, either alone or as concurrent chemoradiation (52.9% vs. 82.9%, p=0.006) (Table 5).
The median follow-up time for NAC group was 48.5 months, during which three recurrences (5.9%) and three tumor-related deaths were recorded. All three patients had only distant metastases. However, there was no recurrence in the patients without adjuvant radiotherapy owing to improved pathologic risk factors after NAC. In PS group, the median follow-up time was 32 months, during which four recurrences (11.4%) and three tumor-related deaths were observed. All four patients also had only distant metastases.
The 5-year disease-free survival rates in NAC and PS groups were 93.3% and 81.5%, respectively (p=0.198), and the 5-year overall survival rates were 92.8% and 91.1%, respectively (p=0.426) (Fig. 1). In addition, there were no differences in survival rate among the three groups (responders vs. non-responder vs. primary surgery patients) (Fig. 2).
DISCUSSION
Prognostic factors for the recurrence of cervical cancer are pathologic findings of parametrial involvement, lymph node metastasis and positive surgical margins,20,21 in addition to tumor size and depth of invasion.22 Larger tumors frequently have higher rates of lymph node metastasis as well as local, regional, and distant failure, and patients with larger tumors have lower survival rates.20,23 Neoadjuvant chemotherapy has shown a high response rate, 53-94%, with complete pathological response rates of 10-13.8%.8,11,24-26 We observed a complete response of 7.1% (3/42), along with significant reductions in tumor size and depth of invasion after NAC compared with the PS group. These results suggest that NAC improved operability in patients with bulky cervical cancer by decreasing tumor size. However, chemotherapy-induced tumor necrosis may result in dense fibrosis and adhesions, which make surgical planes difficult to be maintained.27 This study showed that a higher proportion of patients in the NAC group required blood transfusions. It is inferred that more blood loss may be attributed to tumor necrosis and dense fibrosis after chemotherapy. The postoperative hemoglobin decrease in the NAC group was significantly lower, suggesting that this may have been due to prevention of anticipated blood loss as well as the propensity and variable criteria of the anesthesiologist and/or surgeon. However, more patients successfully underwent laparoscopic radical hysterectomy without conversion into laparotomy. Laparoscopic radical surgery can be undertaken without increase of complication rates in patients with bulky tumors.
While a lower rate of nodal metastasis rate has been reported in patients with locally advanced stage IB-IIB tumors after NAC than in those treated with PS (7-25% vs. 30-34%),7,28,29 the NAC group had no beneficial effect on lymph node metastasis in this study. LVSI and parametrial involvement were also similar in the two groups. Although NAC was less effective in reducing lymph node metastases, LVSI, and parametrial involvement, it was more effective in reducing the size of tumor and the depth of invasion. Therefore, two cycles or doses of chemotherapy might be insufficient for reducing the number of lymph nodes metastases or LVSI. On the other hand, these findings suggest that NAC might be ineffective in the management of high-risk patients with lymph node metastasis. It is important to select appropriate patients who would benefit most from NAC prior to surgery. Patients with age of younger than 35 years and adeno- or adenosquamous carcinoma have been reported to be associated with resistance to NAC,30 however, we found that age and histological type were not associated with poor prognosis, and tumors with larger than 5 cm or FIGO stage IIA had represented rather lower response. Neoadjuvant chemotherapy should be considered in treating younger patients with bulky tumor without anticipating poor response.
Of the patients who received neoadjuvant chemotherapy, 63-81% were treated postoperative concurrent chemoradiation.18,31 In this study, a significantly lower proportion of patients treated with NAC received postoperative radiation (52.9% vs. 82.9%) than those undergoing PS. Despite this difference, the disease-free and overall survival rates in the two groups were not statistically different, although the NAC group had a tendency of higher 5-year disease-free survival rate than the PS group. Also, no recurrence was observed in patients who avoided adjuvant radiotherapy owing to changed pathologic risk factors after NAC. However, as there were no differences among responders and nonresponders of the NAC group and PS group, we postulate that rather good survival rate of the nonresponder group may be attributed to postoperative concurrent chemoradiation. As the present study additionally showed that responders of the NAC group with lower postoperative radiation rates had similar survival rate to the PS group, our results highlights that no accentuation of survival may occur in the responder group even if adjuvant radiotherapy is not added owing to changed pathologic prognostic factors after NAC.
These findings suggest that NAC might be a good treatment option in sexually active, premenopausal women with locally advanced bulky cervical cancer affording better quality of life, by allowing them to avoid postoperative adjuvant radiotherapy. This approach may provide conservation of ovarian and sexual function in these patients without worsening the prognosis.
The limitations of our study were its retrospective design, the small number of patients, and limited long-term follow-up. However, our findings indicate that NAC has an effect on pathologic prognostic factors, allowing patients with locally advanced bulky cervical cancer to avoid adjuvant radiotherapy without worsening their prognosis.



 XML Download
XML Download