

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer is the second most common cancer in women worldwide, with approximately 440,000 cases reported annually.1 Cervical cancer has been the most common cancer among Korean women, but a 2002 report indicated that the number of women with cervical cancer has decreased to less than 10% of the total number of cancers in women, reducing the annual rate of cervical cancer to 20 cases per 100,000 women. However, approximately 5,000 new cases still develop in Korea annually, and about 1,300 of these patients die of the disease.2
One problem with cervical cancer screening is the cost and time that is required for evaluation, treatment, and follow-up.3-7 Under the standard three-step treatment, the appearance of high-grade squamous intraepithelial lesions (HSIL) on a Papanicolaou (Pap) smear usually leads to a cervical biopsy guided by colposcopy. If the histological result of the biopsy is cervical intraepithelial neoplasia (CIN) 2 or 3, loop electrosurgical excision procedure (LEEP) or conization is performed. It is cost-ineffective and time-consuming due to all of the visits required for diagnosis, treatment, and outpatient follow-up. Once a patient has an abnormal cervical cytology, she has to visit an outpatient clinic once for a colposcopy-directed biopsy, and once again for treatment. In addition, if the colposcopy-directed biopsy cannot be performed in the appropriate area, it can affect the prognosis of the patient and make the reliability of biopsy controversial. Even further, patients may suffer from emotional anxiety while waiting for the results of the biopsy. These factors have led to new and alternative strategies for evaluating and treating abnormal cervical cytology.
When a see-and-treat is applied, LEEP can be performed immediately without biopsy if CIN2/3 is suspected at colposcopic examination. The see-and-treat provides an opportunity for patients to be diagnosed and treated in a single outpatient visit. This approach should reduce overall costs, the number of hospital visits, noncompliance, and the patient anxiety.8,9 Although advantageous in certain patient populations, this strategy may result in overtreatment because of the low specificity of Pap smears.
In this study, we evaluated the feasibility of a see-and-treat by dividing patients with abnormal cytology who have undergone LEEP into two study groups, based on whether they were treated with or without colposcopy-directed biopsy. The final histological results of the two study groups were compared.
MATERIALS AND METHODS
1. Study subjects
We conducted a retrospective review of the medical records of 1,011 patients who underwent LEEP at the Department of Obstetrics and Gynecology at Gangnam Severance Hospital from January 2004 to December 2008. Each patient with a diagnosis of abnormal cervical cytology initially underwent colposcopic examination. However, colposcopic examination was also performed in the patients with normal cytology when the patient needed further evaluation due to continuous detection of the human papillomavirus (HPV), or the fear of cancer. "Continuous detection of the HPV" was defined as having two or more HPV DNA positive tests with more than 6 months interval between HPV tests. Study subjects were divided into two groups based on the treatment they received: see-and-treat group (If the colposcopic impression was CIN 2/3, LEEP was immediately performed without processing a colposcopy-directed biopsy), and the standard three-step group (If there appeared a suspected lesion of CIN2/3 at colposcopic examination, colposcopy-directed biopsy was performed. All patients diagnosed with CIN 2/3 in the colposcopy-directed biopsy subsequently received LEEP procedure). We only included the cases diagnosed with CIN2/3 by colposcopy-directed biopsy, and the cases with CIN1 or negative histology by colposcopy-directed biopsy were excluded. The patients with glandular cell abnormalities in cervical cytology and a history of cervical dysplasia/cancer were also excluded. The patients were randomly assigned to one of two treatment protocols, and the decision towards LEEP was not influenced by the extent of cytologic findings.
Colposcopic examination of the cervix was performed after application of 5% acetic acid solution to the ectocervix. In order to have an adequate colposcopic examination, the entire transformation zone, if present, was fully visualized. The LEEP procedure was performed with an electrosurgical unit (Surgitron® FFPF EMC, Ellman International INC., Hewlett, NY, USA), using an appropriate sized wire loop (8, 15, 20, or 25 mm loop bayonet electrodes). The size of the wire loop was chosen on the basis of the colposcopic findings during the procedure. Surgical specimens were stored in a 10% formalin solution and submitted to the Department of Pathology for histopathologic evaluation. Abnormal Pap smears are reviewed by a senior pathologist. All colposcopic examinations and LEEP were performed at our hospital by one gynecologic oncology specialist. The classification of cervical cytology was performed according to the 2001 Bethesda system,10 and the final histological results were reviewed by two gynecologic pathologists. This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital.
2. Clinical data collection
For the study subjects, cervical cytology, colposcopy-directed biopsy, and final histology were recorded. To determine the human papillomavirus (HPV) infection rate in the study group, Hybrid Capture® 2 (HC2) test results were also reviewed.
3. Statistical analysis
The final histological results were classified as Negative (absence of CIN), CIN1, CIN2, CIN3, and squamous cell carcinoma (SCC), and then analyzed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Comparisons between the groups were evaluated by chi-square (χ2) test, and p<0.05 was considered to be statistically significant. In addition, the final histological results were divided into two groups: 1) overtreatment group (final histology ≤CIN1), and 2) correct treatment group (final histology ≥CIN2), and the rate of agreement between the initial and final diagnoses in the see-and-treat and three-step group was compared.
RESULTS
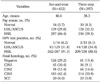
A total of 829 cases were finally included in this study. The clinical characteristics of the study subjects are listed in Table 1. There were 287 HSIL, 129 low-grade squamous intraepithelial lesions (LSIL)/atypical squamous cells of undetermined significance (ASCUS), and 16 normal cervical cytology cases in the see-and-treat group and 236 HSIL, 128 LSIL/ASCUS, and 33 normal cytology cases in the three-step group. The mean ages were 40.6±9.8 years for see-and-treat group and 38.3±9.2 years for three-step group. There were no significant age differences between the groups (p=0.19). In the HC2 test, HPV DNA positivity was 6.1% in normal cytology, 33.1% in LSIL/ASCUS cytology, and 90.1% in HSIL cytology. There was no significant difference in HC2 positivity between the see-and-treat and three-step group (p=0.76).
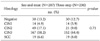
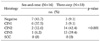
The results of the final histological tests of 523 patients with HSIL cytology who were treated either by the see-and-treat or three-step protocol are presented in Table 2. There was no significant difference in final histology between the two study groups. The final histological results of 257 patients who received LEEP despite LSIL/ASCUS on cervical cytology are shown in Table 3. Patients in the three-step group were significantly more likely to have high-grade histological results (≥CIN2) (p<0.001). In patients with normal cervical cytology, the final histological results showing high-grade lesions (≥CIN2) were also significantly more prevalent in the three-step group (p<0.001) (Table 4).
Fig. 1 demonstrates the rate of agreement between the cervical cytology and final histology in the study groups. In patients with HSIL cytology, the final histological diagnosis was in agreement with initial cytologic diagnosis in 81.9% (235 out of 287 cases) in the see-and-treat group, and 81.4% (192 out of 236 cases) in the three-step group. The rate of agreement between the two study groups was similar (p=0.51). However, in patients with LSIL/ASCUS and normal cervical cytology, the rate of agreement was 17.8% (23 out of 129 cases) and 18.8% (3 out of 16 cases), respectively, in the see-and-treat group, and 63.3% (81 out of 128 cases) and 81.8% (27 out of 33 cases), respectively, in the three-step group. There were significant differences in the rate of agreement between the initial and final diagnosis (p<0.001).
DISCUSSION
See-and-treat approaches are relatively new and have been surrounded with controversy since their introduction. One of the controversies is due to the overtreatment which is partly based on the fact that colposcopy is not a perfect diagnostic test. Data from the ALTS (ASCUS/LSIL Triage Study) trial showed only 15% of women referred with ASCUS cytology had biopsy-proven CIN2/3 (85% over diagnosis). Similarly, women with LSIL cytology had a 25% rate of CIN2/3 (75% over diagnosis).11,12
The risk of overtreatment, or unnecessary treatment, is one of the main criticisms of the see-and-treat approach. The effectiveness of see-and-treat depends on colposcopic impression. Although most studies have found colposcopy to be reasonably accurate compared with cervical pathological diagnosis,13 colposcopy is subject to intra- and interobserver variability, and potentially leads to overtreatment. Thus, patients may be unnecessarily exposed to bleeding and infection, which are the most common complications of the LEEP procedure. Therefore, we recommend that see-and-treat strategy is only appropriate when an experienced colposcopist can differentiate low-grade from high-grade lesions, and the quality of colposcopic practice should be improved by setting appropriate standards.
Recently, strategies have limited the see-and-treat protocol to only patients with HSIL cervical cytology. To decrease the possibility of overtreatment, patients must have a high probability of having CIN2/3 before undergoing the see-and-treat protocol. The use of see-and-treat strategy in a patient population with an HSIL cervical cytology has been shown to decrease overtreatment. Irvin and co-workers reported on a trial that included patients with a Pap smear and colposcopic diagnosis of HSIL.14 Overtreatment was 18% if the threshold included patients with mild dysplasia and those with negative pathology results. Overtreatment decreased to 4% when the threshold was lowered to include only patients with negative pathology results.
Although there are some controversies in the see-and-treat strategy, the necessity of colposcopy-directed biopsy is also controversial. In 2006, Byrom et al.15 performed biopsies guided by colposcopy in the area that was thought to be the most appropriate in lesions of 170 patients with high-grade cytology or colposcopic findings. They simultaneously performed LEEP and compared their histological results. Approximately 70% of the histological results of colposcopy-directed biopsies concurred with the final histological results obtained by LEEP and showed a tendency to under-evaluate the disease. Another study also indicated the disadvantages of colposcopy-directed biopsy.16 They suggested that it did not lower the rate of false positives and therefore could not improve the accuracy of diagnosis. It also delayed the treatment, resulting in increased emotional anxiety in patients.
In the current study, we compared the final histological results of see-and-treat protocol with those of the standard three-step protocol. In our data set, the rate of agreement between initial and final diagnoses was not significantly different only in the HSIL cytology cases, indicating that the addition of a colposcopy-directed biopsy does not reduce the ratio of overtreatment, and has a limited predictive value for the final histological result after LEEP in patients with HSIL cytology. In the HSIL cytology cases, 19 out of 287 patients (6.6%) in the see-and-treat group were diagnosed with invasive carcinoma after LEEP, as shown in Table 2. All patients with invasive carcinoma were immediately treated according to National Cancer Comprehensive Network (NCCN) clinical practice guidelines the next day.
In the LSIL/ASCUS, or normal cytology cases, there were more cases of correct treatment (final histology ≥CIN2) in the three-step group (63.3% in LSIL/ASCUS cytology and 81.8% in normal cytology) than in the see-and-treat group (17.8% in LSIL/ASCUS cytology and 18.8% in normal cytology) (p<0.001). As a result, overtreatment was much more prevalent in the see-and-treat group in patients with LSIL/ASCUS or normal cytology. Therefore, for patients with LSIL/ASCUS or normal cytology, colposcopy-directed biopsy before LEEP can be considered effective. One literature indicates that 5% to 17% of ASCUS and 15% to 30% of LSIL found on Pap smears have associated high-grade dysplasia. In contrast, 70% to 75% of HSIL test results are associated with severe dysplasia and the reproducibility of HSIL is far greater than that of ASCUS.17 Therefore, we did not believe that it was appropriate to perform a LEEP without colposcopy-directed biopsy in patients with low-grade lesions found on cervical cytology.
The see-and-treat strategy was also associated with the lowest cost in the management of HSIL cytology result, producing a 41% cost reduction compared with conventional management of the patients with HSIL.18 In addition, the patient's anxiety may be relieved by assurance from the physician that the lesion has been found and destroyed completely, and will be assessed histologically.9 In surveys based on confidential questionnaires, patients' satisfaction with the see-and-treat strategy was shown to be acceptable.19,20
The current study has several potential limitations that must be considered in the interpretation. One limitation is the retrospective nature of this study, in which the possibility of selection bias increases. Another limitation is the small number of study subjects. Despite these potential limitations, we report that the see-and-treat protocol may be an effective strategy in patients with HSIL on cervical cytology and suggestive of CIN2/3 after colposcopy. However, colposcopy-directed biopsy must be performed before LEEP in patients with LSIL/ASCUS or normal cytology for more accurate diagnosis and prevention of overtreatment.


 XML Download
XML Download