

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer is the second most common malignancy and is the most common cause of cancer-related mortality among Filipino women. Although considered as a preventable disease, the burden of cervical cancer in the Philippines remains to be moderately high, where the cost of nationwide organized cytology screening has been a significant limitation. In a country where existing health infrastructure is not sufficiently developed to support cytology-based screening program, the use of alternative screening modalities, such as visual inspection of the cervix aided by acetic acid (VIA) with or without magnification, is currently under evaluation. In addition, prophylactic human papillomavirus (HPV) vaccination for the prevention of infection and related disease is being considered as an additional cervical cancer control strategy.
BURDEN OF CERVICAL CANCER IN THE PHILIPPINES
According to the Filipino cancer registry 2005 annual report,1 the incidence of cervical cancer remained stable from 1980 to 2005, with an annual age-standardized incidence rate of 22.5 cases per 100,000 women.2 In 2005, there were 7,277 new cases of cervical cancer, with 3,807 reported deaths. The overall 5-year survival rate was 44% and mortality rate was 1 per 10,000 women.1 The high mortality rate was attributed to the fact that 75% of women were diagnosed at late stage disease with treatment being frequently unavailable, inaccessible or non-affordable.
The Philippine General Hospital (PGH) has been the country's government tertiary center reporting the highest number of new cervical cancer cases. In 2006, 466 new cases were reported, of which 68% were squamous cell carcinoma, 21% adenocarcinoma, 3% adenosquamous and 8% of other histology.3 Among these cases, more than half (52%) were diagnosed as stage III (Fig. 1).
HPV PREVALENCE IN THE PHILIPPINES
1. HPV prelavence in cervical cancer
The strong association between HPV and cervical cancer is well established. The reported prevalence of all HPV types is 93.8% in squamous cell carcinoma and 90.9% in adenocarcinomas.4
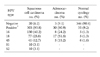
HPV 16 and 18 are the 2 most common HPV types, although HPV 18 alone is relatively more frequent in the Philippines compared to the type distribution estimates in the world. Other common HPV types in decreasing frequency are 45, 52, 51. For women with squamous cell carcinoma, the most common HPV type is 16, followed by types 18, 45, 52 and 51; whereas for women with adenocarcinoma, HPV type 18 is the most common,4 followed by types 16 and 45 (Table 1).
RISK FACTORS FOR HPV INFECTION AND CERVICAL CANCER
Risk factors for HPV infection and cervical cancer in the Philippines are similar to those reported in other countries. The prevalence of some co-factors, including smoking, oral contraceptive use, and fertility, for cervical carcinogenesis in the Philippines5 is shown in Table 2.
A case control study of Ngelangel et al.4 reported that women with less household amenities (a proxy for socioeconomic status), having ever smoked, having given birth 6 or more times and are at a younger age during first intercourse were at an increased risk of squamous cell carcinoma. On the other hand, there was a lower risk of squamous cell carcinoma with decreasing time interval from the last Pap smear. For adenocarcinoma, less number of household amenities, high parity and increased interval from last Pap smear were the identified risk factors.
1. High risk individual sexual health profile
The sexual knowledge and attitudes of the Filipinos contribute to increasing the risk for HPV infection and cervical cancer. Different surveys reveal significant risk behaviors and low knowledge of the Filipinos about sexually transmitted infections (STI). In 2002, freelance Filipino female sex workers admitted having an average of 5 partners per week with only 30% consistent condom use. Most avoid the use of condoms as they ascribe condom use to a lot of myths. These sex workers likewise claim to have little or no knowledge on STI.6
Condom use is equally low among high-risk male individuals. According to a multicenter population based survey by Ramos-Jimenez et al.,7 condom usage is very low among Filipino male sex workers, seafarers and truckers, and its primary usage is as a contraceptive and not as protection against STI.
Overseas Filipino workers (OFW) are also considered vulnerable to STI. These individuals admit to engage in casual sex brought about by factors, such as homesickness, desire for sexual contact, economic pressure to engage in paid sex, and vulnerability to sex trafficking. In most instances, they fail to use condoms.6
2. Adolescent and young sexual health profile
The 2005 World Health Organization-Western Pacific Regional Office (WHO-WPRO) reported the mean age of sexual debut to be 14-15 years. In 2002, 23% of young adults had engaged in premarital sex and the number steadily increased over the last decade. Moreover, about 10% of young women reported that their first premarital sex experience was without their consent.8
Premarital sex initiates and/or accelerates entry into marriage and the Filipino youth marry at an early age. An estimated 1.6 million young adults ages 15-27 years, or 34% of the country's youth, have had multiple sexual partners.8
The prevalence of STIs such as gonorrhea and Chlamydia trachomatis is high among young people. Human immunodeficiency virus (HIV) infection in females occurs at a younger age group compared to males (47% of infected women are between 20-29 years).8
Risky sexual behavior is likewise common among the youth. Only 26% of sexually active adolescents admitted to having used contraceptives, with condom use as the most common method. Of the 78% male adolescents who do not use contraceptives, 6% engage in commercial sex. Similarly, there is an increasing number of female adolescents engaging in unprotected commercial sex (17% in 1994 and 30% in 2002).
Among sexually active adolescents, knowledge on contraception is poor, increasing their risk of exposure to HPV. Of those surveyed, 27% thought that the pill must be taken just prior to or straight after sexual intercourse. Only 4% of young women can be considered knowledgeable on the subject of contraceptives and family planning.8
CURRENT CERVICAL CANCER SCREENING PROGRAMS
The Philippine Department of Health (DOH) has advocated cervical cancer screening, but only less than half (42%) of the 389 Philippine hospitals surveyed offer screening and early detection services for cervical cancer, and only 8% have dedicated screening clinics.2 The 2001/2002 WHO Health Survey reported a dismal 7.7% total Pap smear coverage of Filipino women aged 18-69 years.5
In a study by the University of the Philippines-Department of Health (UP-DOH) Cervical Cancer Screening Study Group (2001), identified causes of failure of cervical screening methods include 1) lack of knowledge about symptoms associated with cervical cancer, 2) a fatalistic attitude towards cancer and lack of awareness that cervical cancer is curable, 3) lack of cytologic screening facilities and expertise and of treatment facilities in rural areas, and 4) lack of patient compliance with follow-up and treatment.9 Only 23% of respondents had received a Pap smear in which 26.6% of these women were from metropolitan Manila and 18.5% were from other areas outside of metropolitan Manila. The women who were more likely to have Pap smears were married, had more children, had a family history of cancer or perceived themselves to be at risk for the disease.
In February 2006, the Philippine DOH established a Cervical Cancer Screening Program to initiate an "organized" nationwide program that includes sustainable capability building, training, educating, and hiring of health workers on proper VIA, Pap smear, cytology, colposcopy, and pathology.10 Considering the low resources, VIA will be advocated as an alternative screening method for cervical cancer, especially in primary and secondary level health care facilities without Pap smear capability, by government health and welfare sectors, nongovernment organizations, professional and civil societies at the national and local levels. Pap smear with VIA triage, colposcopy, tissue biopsy, cryosurgery and surgery treatment [total abdominal hysterectomy (TAH) and total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAHBSO)] will be available at the secondary levels plus radiotherapy and chemotherapy at the tertiary level.10
Recommended screening guidelines are the following: 1) women 25-55 years old will undergo VIA (with acetic acid wash) cervical cancer screen at least once every 5-7 years in areas with no Pap smear capability, otherwise Pap smear will be used; 2) acetic acid wash (3-5%) will be used as the primary screening method at local health units (rural health units; health centers), district hospitals and provincial hospitals with no Pap smear capability; 3) VIA will be used as a triage method before Pap smear at district, provincial and regional hospitals with Pap smear capability; 4) positive or suspicious lesion noted upon screening will be referred immediately; and 5) referral centers for cervical cancer diagnostic tests and treatment will be established in tertiary facilities.10
Although the DOH screening program is not fully implemented as of yet, sustainability of the program will be ensured through local financing, e.g., subsidy from the local government unit or health facility concerned, Philippine Health financing, or fee for service (user fee) scheme. A standard system of recording and reporting will be developed at service delivery facilities in collaboration with population-based cancer registries. Periodic evaluations will be done to assess the quality of VIA being done, and cytology-based centers will be improved and increased as the country's economics improve. In order to target women about cervical cancer screening and services, there will be an annual public education campaign via mass media and interpersonal communication within each health center.
In 2006, the Johns Hopkins Program for International Education on Gynecology and Obstetrics (JHPIEGO) Global Cervical Cancer Prevention launched the JHPIEGO Cervical Cancer Prevention Network Program (CECAP) at the Philippine General Hospital Cancer Institute. The aim of CECAP is to increase education and awareness about cervical cancer in Filipino women and provide them with access and information to screening and effective treatments through single visit approach-VIA screening and treatment with cryotherapy for those positive during the same visit, as well as HPV vaccination.
CERVICAL CANCER PREVENTION AND HPV VACCINATION
1. Vaccine acceptability
Two prophylactic HPV vaccines are registered and marketed in the Philippines that prevent against HPV types 6, 11, 16 and 18 (Gardasil) and against types 16 and 18 (Cervarix).
To determine the acceptability of HPV vaccines in the Philippines, a focused group discussion and exploratory survey was initiated with 195 women with daughters 12-15 years recruited from the Philippine General Hospital Obstetrics-Gynecology charity clinics regarding their knowledge and attitude towards HPV vaccination.11 Only 14.4% of those surveyed had heard of HPV with television being the main source of information and doctors being the second. Approximately 56.4% of the women identified HPV as an STI and only 31.8% associated it to the development of cervical cancer. The HPV vaccine was acceptable to 75.4% of women because it would prevent illness, and of these more than half (55%) thought it should be given prior to sexual activity, while 27% thought it should be administered between 12-15 years of age. Many thought that men should also receive the vaccine to prevent them from infecting their partners.11
Acceptability of the vaccine was higher when respondents were recruited from the Philippine General Hospital general wards. In ten mothers aged 21-43 years, nine mothers would allow their children to receive the HPV vaccine even if only one out of ten knew about it. Likewise, in ten pediatric patients aged 10-19 years, seven would like to receive the vaccine. For those non-acceptors, the reasons cited were young age, painful injection and sexual inexperience.11
Another concern against HPV vaccination is the issue that it could promote or encourage unsafe sexual behavior among adolescents. However the predominant reason for non-acceptance of the vaccine is its high cost.11
2. Vaccination policy and delivery
The Philippine DOH has not formulated a policy on HPV vaccination, perhaps stemming from the most controversial concern that such formal policy could have a negative impact on sexual behavior of the youth. However, it may be worthwhile to consider the impressions from the Report Card-HIV Prevention for Girls and Young Women (the Philippines) as a framework for a prospective Philippine HPV Vaccination Program: 1) minimum legal age at marriage is 18 years; 2) sex work is illegal but tolerated and common in many areas; 3) there is no budget allocation for sexual and reproductive health services, and where such services exist, they tend to be based on marital status that on age-married youths are regarded as adults for whom services are "acceptable", with discrimination against those who are not married; 4) STI treatment is not free, neither is voluntary counseling and testing; and available data suggest that fewer women access STI testing compared to men.12
More young people engage in sex at an earlier and often without contraception. These issues call for a comprehensive evidence-based sexual and reproductive health program that takes into consideration the needs of the youth. It should have a clear guideline, which is national in scope that will provide young people with access to health services. Commitment to women's health should incorporate HPV vaccination into the educational curriculum with learning modules to adequately train teachers. The success of HPV prevention for girls and young women will depend on the political will of the government, as well as the support from relevant inter-governmental and non-government organizations (NGOs), and donors.
3. Research on deployment of HPV vaccination
The current DOH Cervical Screening Program includes Pap smear, VIA, colposcopy and tissue biopsy in women aged 25-55 years. If HPV vaccination is integrated into this program, the target population should be extended to include girls and women aged 11-24 years, and those who have not been vaccinated or have not completed the full course. A national registration system that is linked to a population-based tumor registry could also be implemented to identify a cohort of vaccinated women who can be followed up and compared to unvaccinated cervical cancer cases identified from the tumor registry.
Introduction of an HPV vaccination program can be done in phases across different regions of the archipelago through demonstration research projects. Once the program is operational, evaluation of its short and long-term effects can be done, specifically to evaluate: 1) the knowledge, attitudes, practices and acceptability of vaccination of the target female population and health providers before, during and after implementation to capture behavioral changes and caveats to improve the program and to assess the effectiveness of regular information, education and communications campaigns; 2) the technical issues on vaccine use in the field-vaccine storage, handling, and distribution as well as a nationwide registry; 3) compliance with the three dose vaccine regimen; 4) the health economic impact of vaccination with regard to efficacy and long term safety, and to include the use of new vaccines; 5) the effects on sexual-reproductive health demographics of Filipino adolescents; 6) the effects of cervical screening, although the recommendation for screening has not changed for women who have been vaccinated; and 7) the impact of HPV vaccination on the incidence of cervical cancer. Evaluation of the HPV vaccination program should be spearheaded by the government with collaborative support from local agencies and international research organizations.
The DOH has not received a proposal for the inclusion of HPV vaccination in its relevant public health programs such as the Expanded Program for Immunization, Women's Health and Safe Motherhood Program and Cancer Control Program. School-based programs may be the best way to reach the target youth. In this regard, the Department of Education, Culture and Sports (DepEd) may be involved in the HPV vaccination campaign. DepEd's Population Education Program includes a curriculum on responsible sexual behavior and reproductive health care commencing at the 5th grade elementary school level and up to college. To cover the out-of-school youths that comprise 15% of the 7-24 year age group, community-based programs should be the most appropriate approach.
DIAGNOSIS AND TREATMENT
The Society of Gynecologic Oncology of the Philippines, Inc. (SGOP) provides a clinical practice guideline (CPG) for gynecologic oncologists of the country to standardize diagnosis and treatment of gynecologic malignancies. In the diagnosis and management of cervical cancer, certain general guidelines are recommended: 1) diagnosis of cervical cancer requires a biopsy; 2) staging is based on careful clinical evaluation, which may include proctosigmoidoscopy, cystoscopy, intravenous pyelography (IVP), chest X-ray and skeletal survey, if necessary; 3) additional diagnostic imaging studies, such as ultrasound, magnetic resonance imaging (MRI) computed tomography scan (CT scan), positron emission tomography scan (PET scan), PET CT scan and bone scintigraphy, may be done to guide in treatment planning but not used for staging.13
The standard of treatment for cervical cancer is complete radiotherapy concurrent with chemotherapy (concurrent chemoradiation). However, for patients who are unable to receive chemotherapy, radiation alone is acceptable. For early staged disease, stage IA1-IIA (with tumor size < 4 cm), surgery in the form of extrafascial hysterectomy (for stage IA1) or radical hysterectomy (for stage IA2-IIA) with or without bilateral salpingo-oophorectomy with pelvic lymphadenectomy is recommended. Radical vaginal hysterectomy is also a surgical option but is limited to selected cases of stage IB1-IIA with low risk for parametrial or nodal metastasis, such as tumor size less than 2 cm, no evidence of metastasis by imaging and metastatic work-up, and with pelvic organ prolapse. Subsequently, patients may undergo adjuvant chemoradiation in the presence of surgico-pathologic prognostic factors such as tumor size > 2 cm, cervical stromal invasion greater than 1/3, positive lines of resection, presence of lymph node metastasis, positive lymphovascular space invasion (LVSI), and presence of endomyometrial invasion. The presence of tumor in the vaginal cuff or less than 2 cm tumor free margin requires additional brachytherapy. In the presence of biopsy-proven metastasis, systemic chemotherapy and individualized radiotherapy is recommended.13
1. Treatment outcomes
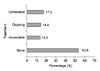
At the Philippine General Hospital, for the year 2008, 75.6% of the new patients seen were candidates for chemoradiation, and only 11.6% were eligible for surgery (Fig. 2).14
Of the patients for chemoradiation, only 17.6% were able to complete treatment. On the other hand, 53.8% were not able to start treatment at all (Fig. 3).14 Treatment-related costs of cervical cancer exceeded twice the average annual income in the Philippines with an average cost of US$350-1,100 for diagnosis and pretreatment evaluation, US$1,100-4,850 for surgery and US$2,100-6,000 for chemoradiation.3
It is uncommon for patients to complete chemoradiation within the recommended period of 55 days (7-8 weeks). Among the patients treated with chemoradiation, only 22.6% were able to complete treatment within 7-8 weeks. Seventy-two percent completed treatment for more than 9 weeks (Fig. 4). The common reasons for prolonged treatment were financial constraints and need to correct treatment-related anemia and electrolyte imbalances. Recurrence or persistence rate of cervical cancer was 37.7%.
CURRENT RESEARCHES IN CERVICAL CANCER
Despite the current advancements in the treatment of cervical cancer, research, particularly those involving radiotherapy use, remains limited due to the economical burden that radiotherapy imposes on the researcher and the institution involved. Radiotherapy studies are generally not encouraging because of the inappropriate delivery of dosimetry due to inadequate facilities, protracted treatment and poor follow-up of patients in a government institution. Studies on chemotherapy are limited by the cost of the medications. In most instances, such studies are generally multicentered and pharmaceutically initiated. Because of such limitations, researches and publications on cervical cancer treatment are redirected more on case reports and case series.
The Philippines has participated in phase II and phase III clinical trials involving both the quadrivalent and bivalent vaccines. It has become the site of multicenter studies notably the ones on radiotherapy concurrent with Capecitabine and another trial concurrent with Ifosfamide. Genotyping studies of preinvasive and invasive cervical cancers are also being conducted. Lastly, registry of HPV warts is being performed by the Asia Oceania (Research Organization on) Genital Infections and Neoplasia, Philippine Chapter (AOGIN-RP).
CONCLUSION
Cervical cancer has remained a leading cancer in women in the Philippines. For close to five decades, standard Pap screening has been available for opportunistic screening, but organized programs have yet to be implemented, largely due to high costs and needs for infrastructure within the health system. Recently, alternatives to Pap smear screening have been introduced, where VIA-cryotherapy programs are being actively evaluated. HPV vaccination has been approved in the Philippines with new efforts to integrate primary prevention at the forefront of cervical cancer control. Since the NIH recommendation in 1999, concurrent chemoradiation is still the standard treatment for cervical cancer. Though it may be a challenge, future directions should be towards improving availability of both preventive and curative measures of cervical cancer management to the general population.




 XML Download
XML Download