

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer is the leading cause of cancer-related death in the female population worldwide. In 2006, about 500,000 cases of cervical cancer were newly diagnosed and more than 280,000 deaths occurred (World Health Organization). During the past 4 decades, the incidence and mortality from cervical cancer have declined significantly primarily because of the widespread use of the Papanicolaou (Pap) test as a screening test to detect cervical abnormalities, and the speed of decline has decreased so that it appears to have plateaued at present. However, a higher incidence rate is still being observed in developing countries.
Human papillomavirus (HPV) is the primary cause of cervical neoplasia. More than 100 types of HPV have been found and are classified as high-risk or low-risk types according to their oncogenicity.1 HPV 16 and 18 cause 70% of cervical cancers, while HPV 6 and 11 cause most of genital warts, or condylomas.2,3 At present, a prophylactic vaccine has been developed and is now utilized worldwide, and there are many ongoing studies for a therapeutic vaccine. It is expected that the incidence of cervical cancer will decrease rapidly in future because of the HPV vaccine.
However, cervical cancer is still a significant problem, especially in developing countries and resource-insufficient areas such as Africa, Asia, Central and South America.4-6 This is partially related to poor availability of health care, which is induced by social and cultural barriers that decrease patient compliance and interrupt physician education.7,8 It is also related to the fact that HPV vaccines will be first introduced into industrialized countries and only later in developing countries. In its aspects of incidence and mortality of cervical cancer, Korea has the pattern of a developing country. In this article, we will first describe the prevalence and risk factors of cervical cancer in Korea, and then will introduce the current situation of cervical cancer prevention and availability of HPV vaccine in Korea.
EPIDEMIOLOGY OF CERVICAL CANCER AND HPV INFECTION IN KOREA
The incidence of cervical cancer in Korea has steadily increased over the past 10 years. Cervical cancer accounted for 9.8% of all new cancer cases in 2002, with approximately 4,500 invasive cervical cancer (ICC) cases and 3,000 carcinoma in situ (CIS) cases being diagnosed.9,10 However, the slope of decline in incidence is not as steep a change as that seen for developed countries. In Cancer Incidence in Five Continents (Volume IX),11 the age-standardized rate (ASR) for cervical cancer in Korea is 15.4 per 100,000. The ASR for cervical cancer in Korea has steadily declined from 19 per 100,000 women in 1993-1995 to 15 per 100,000 women in 1999-2002, while that of adenocarcinoma (ADC) has remained relatively constant (ASR 1.3 in 1993 and in 2002) (Fig. 1).11 Even though the cervical cancer mortality reported by the National Statistical Office has increased, the corrected cervical mortality also shows a decreasing trend, as expected.12 The overall corrected age-standardized mortality rates per 100,000 women declined from 5.2 in 1993 to 3.9 in 2002, while cervical cancer mortality substantially increased in women aged 70 and older.12 Furthermore, according to a recent report on cancer survival using a nationwide population-based cancer registry in Korea (1993-2002), the overall five-year relative survival rate for cervical cancer patients was 78.7% (95% CI, 78.1-79.3) and the trend in cervical cancer mortality in Korea has not significantly changed with time.13
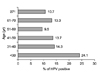
HPV prevalence in Korean women has been investigated in numerous studies. It has been found to be diverse according to age groups, areas, socioeconomic status, and methods for detection of HPV DNA, from 10% to over the range of 40%. However, most reports have shown that the overall prevalence of HPV infection was 10-15%. The incidence of HPV infection was significantly higher in females between 20 and 30 years than in other age groups and the rate of abnormal Pap smears was significantly higher in HPV positive groups than in HPV negative groups. Through the research with women who visited a Health Promotion Cancer study in 2002, Joo et al.14 reported that the overall prevalence of HPV infection was 12.6% (389/3091) and was calculated at 15.5% when standardized. The prevalence of HPV infection was 24.1% (14/58), 14.3% (64/446), 13.7% (165/1206), 9.5% (93/977), 13.3% (50/376) and 10.7% (3/28) in the third, fourth, fifth, sixth, seventh, and eighth decades of age, respectively (Fig. 2). Shin et al.15 interviewed and examined a randomly selected sample of 863 sexually active women (range, 20 to 74 years, median 44) and 103 self-reported virgins from Busan, Korea between November 1999 and March 2000. This reports found that the rate of abnormal Pap smear findings was 4.7% and the overall prevalence of HPV DNA was 10.4%; HPV prevalence was 8.5% among cytologically normal women, 22.2% among those with atypical squamous cells of undetermined significance (ASCUS), 52.9% among those with low-grade squamous intraepithelial lesion (LSIL) and 100% among 7 women with high-grade squamous intraepithelial lesions (HSIL) or worse (Fig. 3). The most common HPV DNA types, in either single or multiple infections, were HPV 70, HPV 16 and HPV 33. Overall, anti-virus-like particles (VLPs) against one or more HPV types were identified in 19.8% of sexually active women. The most frequently found anti-VLPs were anti-HPV 18 (9.0%), anti-HPV 31 (7.6%) and anti-HPV 16 (6.3%). Prevalence standardized by age on the basis of the world standard population was 13.0% for HPV DNA and 17.1% for anti-VLPs. Among 103 virgins, 4.9% had anti-VLPs. Based on 11 published papers,16-26 the most frequent high-risk HPV types among women with normal cytology were HPV-52, 39, 58, 56, and 51. The most common high-risk HPV types in cervical cancer cases were HPV-16, 18, 58, 33, and 35. HPV-16 remains the most common HPV type across the range of cervical lesions.
HPV prevalence in sexually active women ranges from 10% to over 40%. This wide range is at least partially due to the age groups evaluated, their socioeconomic status, and the methods for HPV DNA detection. Bae et al.27 estimated the overall prevalence and type distribution of HPV in Korean women through a literature review and meta-analysis of a total of 18 studies (13,842 cases). The adjusted overall prevalence of HPV infection was 23.9% (95% CI, 23.8-24.1%) in women with normal cytology and 95.8% (95% CI, 95.4-96.2%) in women with cervical cancer. This is higher than the approximately 15% rate seen globally. In cases with low-grade and high-grade lesions, the adjusted HPV prevalence was 60.0% and 85.8%. Type 16 was predominant regardless of cervical disease status, and type 58 occupied significantly larger proportion in high-grade cervical intraepithelial lesions and cervical cancers of Korean women. HPV types 58, 33 and 52 together accounted for about 20% of infections in cervical cancer and high-grade intraepithelial lesions.
RISK FACTORS FOR HPV INFECTION IN KOREA
In Korea, one out of ten women is infected with HPV in the general female population according to two surveys carried out in 2000 and 2002 in the town of Busan. The prevalence was much higher in young women than in middle-aged women.15,28 The International Agency for Research on Cancer (IARC) HPV prevalence survey in Busan, Korea, with a random age-stratified sample of the general female population, revealed that young age, currently smoking cigarettes, having multiple lifetime sex partners and a husband's extramarital relationships were strong risk factors for HPV infection.15,28
HPV is a common pathogen resulting from sexually transmitted infection; therefore, risk factors for HPV exposure are related to patterns of sexual behavior. Young women in South Korea start to have penetrative sex relatively late (median age: 18 years). Table 1 shows the characteristics of selected sexual behaviors and reproductive factors among women in Busan, Korea. These results were obtained from the pooled analysis of three different HPV prevalence surveys in Busan15,28,29 obtained during the period of 1999-2005. However, sexual behaviors of young Korean women have been changing rapidly as the western life has become fixed during the last century. A recent second online survey for the health behavioral factors among adolescents, including 80,000 junior and high school students, showed that mean age at sexual debut was 14.2 years old and less than 40% of these young people used contraceptive methods for penetrative sexual intercourse.30 The young people of this generation seem to have different concepts of sexual behavior compared with the past generations, and these changes influence HPV exposure and the prevalence of cervical cancer.
According to reports from The Korean Society of Preventive Medicine, risk factors for cervical cancer in Korea are socioeconomic status, familial history, number of sexual partners, and age at first sex, etc. In females with a history of pregnancies, the risk of developing cervical cancer is 5 to 6 times greater compared with that of a nullipara. If there is familial history of cervical cancer, the risk is 2 times greater. An increased risk of cervical cancer is also associated with age at first sex at less than 20 years old.31
CURRENT SITUATION OF CERVICAL CANCER SCREENING IN KOREA
The Pap test is still the most common cancer screening test in Korea despite it being 50-year old technology. Cervical cancer screening with the Pap test was first introduced in the late 1950s in Korea and adopted as a Health Screening for Medical Insurance Beneficiaries as of 1988; however, the Pap screening rate has been kept at very low level; about 34% in 1998 (in women age 20 and over, ever screened during the last 2 years). In 1999, the National Cancer Screening (NCS) Program was started only for Medicaid for stomach, breast and cervical cancers, which was extended in 2002 to those with the lower 20% premium of the National Health Insurance Corp (NHIC). The Korea Health Insurance Corp. covered cervical cancer screening in 9.6% of the target population in 2001, and this proportion has been increasing stepwise. The NCS Programs have expanded their target population as well as target diseases and, at present, support cancer screening tests to those on Medicaid and those with the lower 50% premium of NHIC for stomach, breast, cervical, hepatic and colorectal cancers. According to the National Health and Nutrition Survey, the overall participation rate for cervical cancer screening was estimated at approximately 40% and showed an increase from 22.4% in 1998, 39.8% in 2001, to 41.5% and the participation rate was the highest in women aged 40-49 years between 2001 and 2005. In a recent telephone survey,32-34 the overall participation rate in a cervical cancer screening program within two years was 55-58% during the year 2004-2006.
The Ministry of Health & Welfare presented guidelines for cervical cancer screening in Korea, as the National Cancer Screening (NCS) Program. Its basic principles are as follows: the main screening tool is the Pap test conducted by gynecologists, and targets all women age 30 and over, who are followed every 2 years (Table 2). This guideline is different from several consensus guidelines developed worldwide in many aspects; the target population is older, the testing interval is longer and there is no recommendation for a HPV DNA test. In fact, the Korean Society of Obstetrics and Gynecology recommends another cervical cancer screening schedule: a Pap test every a year for women 21 years and over (Table 2). However, the National Cancer Screening Program should be planned considering availability and cost-effectiveness in order to maximize its own efficacy; therefore, it can be different from the guidelines of an academic society.
In a meta-analysis of 94 studies,35 the sensitivity of Pap testing ranged from 30 to 87%, and the specificity ranged from 86 to 100%. Shin et al.36 reported 71.2% sensitivity and 97.7% specificity in Korea through an analysis comparing cervical cytology versus histological findings of 1,023 women. Another study reported that the sensitivity of the Pap test ranged from 70.5 to 83% in Korea; however, the results showed diversity according to institution.37 A number of factors, including small lesion size, inadequate sampling, obscuring blood and debris, and results specific to individuals, limit the sensitivity of the conventional Pap test. In an attempt to improve sample quality, interest has focused on liquid-based cytologic preparations.38 This does not yet apply to screening methods in Korea, but its utilization is rapidly increasing.
A number of studies have examined HPV testing as a primary screening tool in both developed and developing countries and have used a number of techniques for HPV detection, including hybridization methods and polymerase chain reaction (PCR) analysis.39-43 A meta-analysis of HPV testing as the screen for cervical cancer found that it was more sensitive than cytology, but HPV testing had a somewhat lower specificity. The average sensitivity for detection of high-grade disease with primary HPV testing was 85% with a specificity of 84%.
HPV DNA tests have not been permitted as a screening test for cervical cancer in Korea. However, the NHIC has approved HPV DNA testing to confirm cervical dysplasia or carcinoma following an abnormal Pap smear.
HPV VACCINATION IN KOREA
There are two cervical cancer candidate vaccines. The quadrivalent vaccine, Gardasil™ (Merck & Co., Inc., Whitehouse Station, NJ, USA), consists of a mixture of four recombinant HPV type-specific VLPs composed of the L1 major capsid proteins of HPV types 6, 11, 16, and 18 synthesized in Saccharomyces cerevisiae. The four VLP types were purified and adsorbed onto aluminum hydroxyphosphate adjuvant [Al (OH)3]. The bivalent vaccine, Cervarix™ (GlaxoSmithKline Biologicals, Rixensart, Belgium), consists of a mixture of two recombinant HPV type-specific VLPs composed of the L1 major capsid proteins of HPV types 16 and 18 synthesized in a baculovirus. Cervarix™ has an ASO4 adjuvanted system that is composed of monophosphoryl lipid A and aluminum hydroxyphosphate.44,45 In several phase III randomized controlled clinical trials,46-48 the quadrivalent vaccine and bivalent vaccine showed prophylactic efficacy of more than 90% against persistent infection by HPV, abnormal cytology, and cervical intraepithelial neoplasia associated with HPV16 or HPV18 (Table 3). Therefore, these could be used for cervical cancer prevention.
The Korean Food and Drug Administration (KFDA) approved Gardasil™ for the prevention of cervical cancers and genital warts in June 2007 and Cervarix™ for the prevention of cervical cancers in July 2008. Many factors should be considered for determining guideline of routine HPV vaccination; for example, the period of prevention for HPV infection through vaccination, the mean age at sexual debut, the effective time of injection and national financial affairs. If the age of routine vaccination is early, the possibility of prevention of HPV infection might be higher, however the cost for a booster injection could increase. Even if it is the most desirable that HPV vaccination be included in a school immunization program, this is impossible at present because of the high cost. Therefore, it is important to consider the age at sexual debut and the cost-effectiveness within national financial affairs or private medical insurance. There is no financial support at present for HPV vaccination from any national policy in Korea. Considering the amount of information about HPV vaccine and the special conditions in Korea, a clinical guideline for HPV vaccination for prevention of cervical cancer was recommended by KSGOC (Table 4).
CONCLUSIONS
Cervical cancer remains a significant cause of cancer-related deaths in women worldwide, especially in Asia and including Korea. However, screening tests for cervical cancer have reduced the disease burden by up to 75% in countries that have carried out excellent screening programs. A quadrivalent HPV vaccine and a bivalent HPV vaccine have been developed for the prevention of cervical cancer related HPV infection and the use of these has now been approved in Korea. However, many people are not familiar with the HPV vaccine primarily due to high costs and lack of adequate understanding. Therefore, increased disease awareness and utilization of screening is the first priority for controlling cervical cancer. Following this, it will be important to establish effective strategies to obtain funding for HPV vaccination, in addition to the efforts to decrease the cost of vaccination. In the future, cervical cancer is expected to disappear throughout the world in much the same manner as polio has through vaccination programs.






 XML Download
XML Download