

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cancer is not rare in younger women of reproductive age. Recent data estimate that more than 679,540 women in United States, many of reproductive age, are diagnosed with invasive cancer annually.1 The number of young women diagnosed with cancer has been increasing. According to the 2002 Annual report of the Korea Central Cancer Registry, 10,945 reproductive aged women (15-44 years old) were newly diagnosed with invasive cancer in 2002.2 Advances in the diagnosis and treatment of childhood, adolescent and adult cancer have greatly increased the life expectancy of premenopausal women who have overcome their disease. By the year 2010, as many as 1 in 250 patients will have survived malignancies.3 For the treatment of cancer, aggressive chemotherapy, especially with alkylating agents and ionizing radiotherapy, can destroy gonads and subsequently lead to a loss of fertility and premature ovarian failure.4 Even in those patients who were not sterilized by high dose chemotherapy or radiotherapy, there may be an increased risk for complications during pregnancy such as early pregnancy loss, premature labor, and low birth weight.5 It had been reported that a four-fold increased risk of premature ovarian failure (POF) in teenagers treated for cancer, and a risk increased by a factor of 27 in women between 21 and 25 years of age.6
The advent of in vitro fertilization (IVF) and its current worldwide use has resulted in the development of successful cryopreservation techniques for surplus embryos. These cryopreservation techniques have further been applied to the unfertilized mature human oocyte7 and ovarian tissue.8-10
In this brief review, we address which reproductive technologies, especially cryopreservation, are presently available for the preservation of fertility in the reproductive age women who will be treated with an anti-cancer chemoradiotherapy, and some of the challenges encountered with their clinical application.
STRATEGIES TO PRESERVE FERTILITY
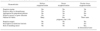
Several options are currently available to preserve fertility in cancer patients and give them the opportunity to conceive when they have overcome their disease: embryo cryopreservation, oocyte cryopreservation or ovarian tissue cryopreservation (Table 1).11-15 The choice of the most suitable method for preserving fertility depends on different parameters: the type and timing of chemotherapy, the type of cancer, the patient's age and the partner status.
If the patient has a partner or accepts donor sperm, embryo cryopreservation should be considered first, since this is a clinically well-established procedure. Embryo cryopreservation is the preferred method to preserve fertility due to reasonable delivery rates, according to the Ethics Committee of the American Society for Reproductive Medicine.16 This method requires the patient to be of pubertal age, have a partner or use donor sperm, and be able to undergo a cycle of ovarian stimulation. However, many women who are faced with a decision regarding their future fertility may not have an established partner or may not desire to use donor sperm.17 In addition, it is not possible when the chemotherapy has to be initiated immediately or when ovarian stimulation is contraindicated due to the type of cancer.
Cryopreservation of oocytes can be used in single women who can undergo a stimulation cycle, although the effectiveness of this technique is very low, with pregnancy and delivery rates ranging from 1 to 5% per frozen oocyte.18-20
Ovarian tissue cryopreservation is the ideal option for prepubertal girls, and for women who cannot delay the start of chemotherapy. Ovarian tissue can be frozen using different categories: cortical fragments, whole ovary with its vascular pedicle or isolated follicles. In humans, ovarian tissue cryopreservation and transplantation procedures have so far been almost limited to avascular cortical fragments, both in experimental and in clinical studies. Until now, ovarian cortical tissue cryopreservation is the only procedure that has resulted in live births in humans after autologous transplantation.14,21,22
1. Embryo cryopreservation
Embryo cryopreservation is an established clinical procedure, and currently is the only widely available option for fertility preservation. Reported survival rates per thawed embryo range between 35 and 90%, implantation rates between 8 and 30%, and cumulative pregnancy rates can be more than 60%.23 However, there are several limitations in this approach. First, the patient needs a male partner or to use donor sperm. Second, ovarian stimulation precedes oocyte retrieval for IVF, necessitating a delay in the initiation of chemotherapy or radiotherapy that may not be acceptable in many cases. Third, exposure to the high serum estrogen concentrations during ovarian stimulation may be contraindicated in women with estrogen-sensitive malignancies such as breast cancer.24 Natural cycle IVF could avoid this high estrogen milieu, but the oocyte yield is too small to use considering the limited time for IVF treatment. Tamoxifen has been used with some success as an alternative to provide safer ovarian hyperstimulation for breast cancer patients.25 However, as tamoxifen has a stimulatory effect on the endometrium, it cannot be used for ovarian stimulation in endometrial cancer patients. Instead, the use of aromatase inhibitors has been proposed for patients with endometrial cancer. Letrozole, a potent third generation aromatase inhibitor, competitively inhibits the activity of aromatase and has a half life of approximately 48 hours.26 Recent studies showed successful ovarian stimulation with letrozole and gonadotropins with reduced estrogen exposure, compared with standard stimulation cycles in breast and endometrial cancer patients.27,28
2. Oocyte cryopreservation
Embryo cryopreservation may not be an option for single women unless they choose to use sperm donation. In these patients, if they have time to complete ovarian stimulation prior to cancer therapy, cryopreservation of mature or immature oocytes can be considered as another option. However, oocyte cryopreservation also delays cancer therapy because it requires ovarian stimulation before obtaining oocytes. In addition, early results have been disappointing with respect to low survival, fertilization, and pregnancy rates after IVF of thawed oocytes, due to the fragility of the meiotic spindle and the formation of ice crystals.23 Thus, it still requires further investigation for this to become a routine clinical procedure.
1) Mature oocyte cryopreservation
Since the first human live birth from cryopreserved oocytes was reported in 1986,29 more than 300 babies have been born with cryopreserved-thawed oocytes. The mature oocyte is extremely fragile during freezing-thawing due to its large size, high water content, and chromosomal arrangement. At metaphase, chromosomes are arranged in a linear fashion at the equatorial plane on meiotic spindles. Intracellular ice formation associated with the freeze-thaw process has been found to be detrimental to the spindle apparatus.30 These characteristics of mature oocyte are the reason for low survival rates after cryopreservation. Sonmezer and Oktay reviewed data from 21 studies in peer-reviewed journals and found a mean survival rate of 47%, a mean fertilization rate of 52.5%, and a mean pregnancy rate per thawed oocytes of 1.52%.23 However, recent advances in freezing and thawing technology resulted in a higher survival rate of frozen-thawed oocytes, as well as improved pregnancy rates.31 One of the factors that improved fertilization rates of cryopreserved-thawed oocytes is the use of intracytoplasmic sperm injection (ICSI) to overcome the zona hardening caused by the cryopreservation process.32 It also has been showed that ICSI results in embryos with greater cleavage rates.33
Based on different rates of freezing and thawing and cryoprotectants used, several protocols for oocyte cryopreservation have been described. The most commonly employed is the slow freeze-rapid thaw protocol. Also, newly developed techniques in oocyte cryopreservation by a slow-freezing protocol include modification of cryoprotectant solution and cryopreservation techniques, and the use of sodium-depleted media.34-37
An alternative technique aimed at preventing ice formation and improved oocyte survival is vitrification. Vitrification is the process of cryopreservation using high concentrations of cryoprotectant with a high cooling rate to solidify the cell into a glass-like state without causing ice formation.38 Vitrification is easier and less expensive and does not require a programmable freezer that is mandatory for the conventional slow freezing method.39 Recently, improved post-thaw survival and fertilization rates and live births have been reported.40 Based on a review of published reports using vitrification, mean survival rate of 68.4%, fertilization rate of 48.5% and pregnancy rate of 1.7% per vitrified-thawed oocyte were reported.23
2) Immature oocyte cryopreservation and in vitro maturation
Immature oocytes cryopreserved at the germinal vesicle (GV) stage survive better than those frozen at the metaphase II stage.41 They are more resistant to damage from cryopreservation because of lower cell volume and lack of a metaphase spindle. However, although GV oocytes have a higher post-thaw survival rate and a lower incidence of spindle damage, the inefficiency of established in vitro maturation protocols results in a final yield of mature oocytes that is similar to that obtained with cryopreserved mature oocytes.42 Recently, similar rates of maturation, fertilization, and embryo development have been achieved by vitrification of immature human oocytes, compared with control oocytes.43 However, only a few pregnancies have been reported using frozen-thawed human immature oocytes and the experience in human GV oocyte freezing is very limited.44,45 The Practice Committee of the American Society for Reproductive Medicine recommended that oocyte cryopreservation should be presently considered as an experimental technique, only to be performed under an institutional review board-approved investigational protocol.46
3. Ovarian tissue cryopreservation
In 1994, Gosden et al. reported the successful restoration of fertility by autografting frozen-thawed ovarian tissue in sheep.47 Due to the recent development of more effective cryoprotectants such as ethylene glycol, dimethyl sulfoxide (DMSO), and propanediol, animal studies were repeated and successful deliveries were reported in a number of species.47,48 In ovarian tissue cryopreservation, hundreds of primordial follicles containing immature oocytes, unlike with embryo or oocyte cryopreservation, can be cryopreserved in situ. There are several advantages, such as abundant germ cells, no need for ovarian stimulation and consequent delay in initiating cancer treatment. Moreover, primordial follicles are significantly less susceptible to thermal injury than both mature and immature oocytes, because of their small size, slower metabolic rates, and the absence of a zona pellucida.24 Similar to oocyte cryopreservation, a male partner is not required. Thus, this procedure is an option for single patients and prepubertal girls. In children, ovarian tissue cryopreservation is the only fertility-sparing method because ovarian stimulation and oocyte collection cannot be considered ethical.
Three strategies, such as fragments of cortical tissue, isolated cryopreserved primordial follicles, and the transplantation of cryopreserved whole ovary, will be discussed.
1) Fragments of cortical ovarian tissue
Since it has been demonstrated that normal menstrual function could be restored and spontaneous pregnancies achieved after autologous orthotopic transplantation of cryopreserved ovarian cortex tissue using oophorectomized sheep,47 ovarian tissue has been successfully cryopreserved and transplanted into many species such as rodents, sheep, and marmoset monkeys.49-51 In a primate, Lee et al. reported that in the successful fertilization and pregnancy after oocyte collection from fresh transplanted ovarian tissue, the graft tissue functioned without any surgical connection to major blood vessels.52 The outer cortical layer of the ovary contains most of the primordial follicles. The ovary is removed by laparoscopy or laparotomy, and cut into strips of tissue around 1-3 mm in thickness and up to 1 cm2 in total area to allow for adequate penetration of the cryoprotectant solution.53 In cancer patients, a pathologic assessment of the ovarian tissue must be performed to exclude the presence of metastatic disease. In in vitro studies, viability can be obtained in over 70-80% of the specimens using the slow freezing and rapid thawing method.
There are, theoretically, three approaches in the development of immature follicles: autotransplantation (orthotopically or heterotopically), xenotransplantation, and in vitro culture.54
Reported cases of autotransplantation of cryopreserved ovarian tissue, either orthotopically within the pelvis of heterotopically within subcutaneous tissue, are summarized in Table 2. There are some different characteristics between orthotopic and heterotopic autotransplantation (Table 3). Orthotopic autotransplantation of cryopreserved ovarian tissue may result in a natural pregnancy if the fallopian tubes remain patent. However, this procedure requires abdominal surgery and general anesthesia. A laparoscopic surgery makes this procedure less invasive but technically more difficult. Several cases have been reported, showing spontaneous follicular maturation23,55 and presumably ovulation following stimulation with menopausal gonadotrophins.23
The first case of a successful spontaneous pregnancy from cryopreserved ovarian cortical tissue has been contended for not providing definite evidence of a pregnancy from cryopreserved and transplanted ovarian cortical tissue, because the subject patient had not undergone a bilateral oophorectomy.21 The major disadvantage of transplanting ovarian cortical strips is that revascularization of the graft needs the several days. Also, the consequent ischemia is the technical limitation of cortical tissue transplantation, whether orthotopic or heterotopic. There is a possibility of follicle atresia during the period of ischemia, before the tissue becomes revascularized. Because of that event, ovarian function might be compromise beyond several months of follow-up (mean duration; 9 months).23,55
Heterotopic autotransplantation of cryopreserved ovarian tissue has several advantages. This procedure is minimally invasive, reversible, repeatable, and it permits easy access to the graft for monitoring the follicular development or in the event of reoperation.56 Usually, heterotopic transplantation can be conducted at sites such as the forearm or abdominal subcutaneous tissue.57,58 It has been claimed that oocyte quality might be compromised by transplantation to a heterotopic site, due to differences in temperature and pressure which may interfere with follicular development in these sites.59 The comparison of the methods of autotransplantation is summarized in Table 3.
In vitro maturation and ovarian tissue xenotransplantation may someday become common applications in conjunction with ovarian cryopreservation. Xenotransplantation of human ovarian tissue was reported in 1998.60 It was revealed that human ovarian tissue xenografted into the severe combined immunodeficiency disease (SCID) mouse demonstrated estradiol production and estrogenization of tissues after follicle-stimulating hormone administration. However, possible transmission of prions and animal viruses accompanying the retrieved oocyte must be considered. Nowadays, this technique is suggested as a means of evaluating follicular reserve and function in cryopreserved human ovarian tissue.61,62 In in vitro maturation of oocytes, epigenetic abnormalities secondary to methylation defects may be of significant concern.63
2) Isolated primordial follicles
Because the oocyte of the primordial follicle contains a relatively inactive metabolic status, as well as a lack of the meiotic spindle, zona pellucida and cortical granules, the primordial follicle is resistant to cryoinjury. Moreover, the small size of follicles facilitates penetration of the cryoprotectant. Despite these advantages, the technique of isolation primordial follicles remains difficult,64 and it has not been possible to culture isolated human primordial follicles to the mature oocyte stage in vitro.65 This method may exclude the possibility of reintroducing tumor cells into cancer patients by autografting of ovarian tissue.
Encouraging the clinical application of this method, further studies are clearly needed to identify factors sustaining follicular growth and maturation in in vitro culture systems.66 Follicle isolation, or partial follicle isolation, severely impairs follicular viability in cultures. After isolation procedure, primordial and primary follicles degenerate within the first 24 hours of culture.67 Therefore the isolation procedure of primordial follicles, using enzymatic digestion, should be optimized to enhance the retrieval rate and viability of the oocyte.
It has been suggested that transplanting a suspension of isolated follicles may be another option, as the follicular basal lamina encapsulating the membrana granulosa excludes capillaries, white blood cells and nerve processes from the granulosa compartment, and grafting fully isolated follicles may be safer.68 In addition, establishing faster angiogenesis and minimizing ischemic and reperfusion damage would permit the introduction of a high number of follicles into the host.
3) Whole ovary
The survival of transplanted ovarian tissue is completely dependent on the establishment of neovascularization. If this process is incomplete, a large proportion of follicles are lost as a result during the initial ischemia period just after transplantation.69,70 It is necessary to maintain the follicular reserve and extend the life span and function of the ovarian tissue so that the ischemic period between transplantation and neovascularization be reduced. One of the future approaches to preserve fertility is the transplantation of an intact ovary with vascular anastomosis, allowing immediate revascularization of the ovary.
Transplantation of fresh whole ovary with vascular anastomosis has already been successfully performed in rats,71 rabbits,72 sheep,73 dogs,74 monkeys75 and humans.76 The first case of restoration of fertility after whole frozen ovary transplantation was reported by Wang et al. in 2002.71 They described that the survival rate was 57% (4/7 rats), which survived for ≥60 days, and the pregnancy rate was 25% (1/4 rats). Despite this success in rats, it remains as a technical problem to cryopreserve whole ovaries from large mammals and humans, which are larger and more fibrotic. There is a difficulty of adequate diffusion of cryoprotectants into large tissues, and vascular injury caused by intravascular ice formation. The duration of subsequent ovarian function is initially limited, mostly due to ischemia resulting from thrombosis.77 To overcome this problem, it has been suggested that the graft be perfused with heparinized Ringer's solution, followed by perfusion and immersion in a bath containing cryoprotectants immediately after oophorectomy. The ovarian vessels and excess hilar tissue is dissected, and grafts are perfused via the ovarian artery with the cryoprotectants using infusion system to maintain a flow rate at 1.3 mL/min with continuous replenishment of the reservoir.78 Recently, such attempts have been also applied in human whole ovary and a comparable survival rate (75.1%) is obtained.79,80
It should be considered in whole ovarian cryopreservation used for younger women, whose ovaries have a mean size of 3×2×2 cm, that this protocol will need a larger cryovial than conventionally used. Also, the programmed freezer system should have a larger cryochamber. Surgical technique should be trained; great care must be taken to remove the ovary, together with a larger part (≥5 cm) of the infundibulopelvic ligament, allowing dissection of the ovarian vessels, and perfusion with a cryoprotective medium. Until now, the status of whole ovary cryopreservation remains experimental. Research and development of technology to cryopreserve whole organs, as well as surgical techniques for the autotransplantation of an entire ovary with its vascular pedicle, should be encouraged.
SAFETY
1. Reimplantation of the primary cancer
Shaw et al. reported the transmission of lymphoma via grafts of ovarian tissue from diseased donor mice to healthy recipients.81 This study emphasized the risks of clinical application by transplantation of ovarian tissue to women recovering from cancer, especially a blood-borne cancer.81,82 However, clinical ovarian metastasis is rare in "common" cancers of young patients, such as Wilms' tumor and Hodgkin's disease. The risk of transferring cancer cells depends on the disease type, activity, stage, and mass of malignant cells transferred. Screening methods should be developed to eliminate the risk of cancer cell transmission with reimplantation. Recently, it has been suggested that preoperative imaging prevents operation and storage of tissue with cancer, and evaluation of stored ovarian tissue for minimal residual disease (MRD) using sensitive markers (e.g. Anti-CD 30, and anti-Ki 67) is essential to increase safety and to prevent reimplantation of tissue with malignant cells.83 In fact, it may be feasible to screen the harboring metastatic cancer cells in the preserved ovarian tissue before transplantation using immunohistochemistry, flow cytometry, or molecular genetic techniques such as reverse transcriptase-polymerase chain reaction and fluorescence in situ hybridization.
2. Lifespan of transplant ovarian tissue
The lifespan of transplant ovarian tissue is dependent on the degree of ischemia. Ischemic injury after transplantation can be minimized by relief of hypoxic tissue damage by using antioxidants and facilitation angiogenesis by angiogenic factors. Ultimately, to prevent ischemic tissue injury, the strategy is whole ovary transplantation with vascular anastomosis. These studies have been conducted to establish the optimal techniques of whole ovaries.
3. Malignant transformation of transplant tissue
The point that needs consideration is that the malignant transformation of transplanted ovarian tissue may occur. The major indications for ovarian tissue harvest are for cancer, and they also have the same risk of cancer in ovarian tissues as well as other tissues. In particular, patients with BRCA-1 and BRCA-2 mutations have a 60% and 10-20% lifetime risk of developing ovarian cancer, respectively.84 These patients often undergo prophylactic oophorectomy to decrease their chance of ovarian / peritoneal cancer by 90%, or as part of a treatment plan for breast cancer.85 Heterotopic transplantation can be considered in these patients, but the transplanted ovarian tissue should be removed in its entirety as soon as treatment for fertility is complete.
In vitro maturation and xenotransplantation may become an alternative plan in the future. However, recent studies have investigated the integrity of human oocytes obtained after subcutaneous xenografting of cryopreserved ovarian tissue into SCID mice and in vitro maturation of retrieved cumulus-oocyte complexes.86 Unfortunately, some oocytes showed abnormal nuclear and cytoplasmic maturation by immunocytochemical analysis of microtubules and DNA.
A completely unknown variable requiring long-term follow-up is the questionable relative risk of epithelial or germ cell malignant transformation in transplanted ovarian tissue secondary to the rapid temperature changes and exposure to cryoprotectants inherent in the cryopreservation process.
4. Trans-species viral infections in xenotransplantation
This technique has additional risks. The epigenetic abnormalities secondary to methylation defects may be of significant concern.63 Xenotransplantation may have a risk of transmission of prions and animal viruses accompanying the retrieved oocyte. in vitro maturation and ovarian xenotransplantation may one day become common applications in conjunction with ovarian cryopreservation, and the practitioner should be able to explain the risk of this techniques.
ETHICAL ISSUES
Young cancer patients are psychologically vulnerable, when they recognize the disease as well as a possibility of infertility after cancer therapy. In this situation, it is important that the physician reassure the patients suggesting several options to preserve their fertility. Moreover, clinical experience is also limited and this technique remains still experimental. Clinical application of these unproven experimental procedures can be ethically complex. The ethical issues of fertility preservation should be discussed.
The primary ethical consideration is the safety of the procedures. The procedure of fertility preservation should not harm the patient by dangerously delaying cancer treatment. For example, oocyte cryopreservation requires ovarian stimulation and oocyte retrieval, which can delay chemotherapy and increase the chance of cancer growth and metastasis. Ovarian stimulation with gonadotropin may increase the E2 levels, which might stimulate estrogen-sensitive tumors (e.g. breast cancer). It is not ethical to suggest oocyte cryopreservation to preserve fertility, because of the risk is clear and the benefit is uncertain. One of the most important ethical issues is to ensure that no remnant cells are reintroduced by subsequent transplantation.
Until now, most strategies to preserve the fertility in women are still experimental and do not guarantee the recovery of fertility. Oocyte and ovarian tissue cryopreservation before cancer therapy appear to be hopeful options for fertility preservation. However, oocyte cryopreservation is not a well-established method and the pregnancy rates are still low. The principles of beneficence and non-maleficence are paramount in the treatment of minors, especially when they are psychologically vulnerable. It should not be offered if delaying anti-cancer therapy would increase the risk of disease aggravation.
Ovarian tissue cryopreservation is also ethically challenging. This method is potentially useful, but it is too early to determine the true benefits since there are only three case reports of live birth after transplantation of cryopreserved human ovarian tissue. Therefore, it is an ethical dilemma whether we should even offer a new, unproven technology with potential benefits but with known risks. Ovarian tissue cryopreservation may increase the risks because it requires surgery under the general anesthesia to harvest ovarian tissue. There would be added risks such as bleeding, infection, and bowel injury. It may not be justified to collect ovarian tissue from infants or very young children whose ovaries are small and for whom surgery is a high risk procedure. It also may not be ethical to offer this procedure to the patients whose ovaries are already exhausted of oocytes because of age or cancer therapy.
In children suffering from cancer, patients' rights may be a concern. In the current context, her 'best interest' includes both her present interest in minimizing risk and her future interest in fertility preservation. This consent should be a reflection of the parents' respect for their child. Children should be allowed to assent to their treatment after being provided with a full explanation including risks, discomforts, benefits, and alternatives. If the medical risk is acceptable, it seems that parents have an ethical right to request fertility preservation.
Knowing that there are options for fertility preservation can be a relief for them, but they should be well informed to prevent false expectations as well as the possibility of being exploited by the commercial interests of the purveyors of unproven technologies.
CONCLUSION
In general, young female cancer patients are poorly counseled on their options for fertility preservation. Treatment of the cancer is of utmost importance, but several assisted reproductive technologies can provide relief from the uncertainty of future without compromising cancer treatments. The number of options is growing continuously, some are more established, such as embryo cryopreservation, and some are still experimental, such as ovarian tissue cryopreservation.
The different cryopreservation options available for fertility preservation in female cancer patients are embryo, oocyte, and ovarian tissue cryopreservation. Because of the variations in the type of cancer, type and dose of chemotherapy, the time available before onset of treatment, the patient's age, and the status of partners, each case should be individualized and requires a different strategy in fertility preservation (Fig. 1).
Under the ethical principle, appropriate expansion of the indication and further studies on optimizing technique must continue in anticipation that cryopreservation of the oocyte and ovarian tissue will become a useful and widely accepted option in preserving female fertility in young cancer patients.



 XML Download
XML Download