

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common cancer in women that is a major cause of morbidity and mortality, with more than 1 million new cases and 410,000 deaths reported worldwide each year.1,2 The primary aim of treatment for early or advanced breast cancer is to maximize therapeutic effect and prevent recurrence through primary surgery followed by adjuvant therapy including chemotherapy, irradiation, or hormonal therapy. In recent decades, tamoxifen, the selective estrogen receptor modulator, has been the standard regimen of adjuvant hormonal therapy for estrogen receptor (ER) positive breast cancer in both pre- and post-menopausal women. Although tamoxifen is an ER antagonist in breast cancer, which reduces the breast cancer recurrence rate and mortality rate,3 it also acts as an ER agonist in other tissue such as the endometrium and ovary. This agonist effect can stimulate proliferation, which increases the risk of polyps, hyperplasia, endometrial cancer, and ovarian cyst formation.4-7
Aromatase inhibitors (AIs) such as anastrozole have been found to be at least as effective as tamoxifen in the treatment of postmenopausal women suffering from ER-positive breast cancer.8,9 Estrogen ablative therapy with anastrozole may not only be effective in the treatment of breast cancer, but may also be beneficial in reducing the risk of other estrogen-dependent diseases.
The aim of this study was to investigate the effect of tamoxifen and anastrozole on the endometrium and ovary in women undergoing adjuvant hormonal therapy after breast cancer surgery.
MATERIALS AND METHODS
Between January 2003 and December 2006, 207 women with ER-positive, primary breast cancer, who were receiving adjuvant tamoxifen or anastrozole treatment more than one year after surgery were included in this study. These women were identified by retrospective review of their medical records and classified into three groups; 155 premenopausal women receiving tamoxifen (group 1), 32 postmenopausal women receiving tamoxifen (group 2), and 20 postmenopausal women receiving anastrozole (group 3). All premenopausal women received adjuvant chemotherapy before tamoxifen therapy. Tamoxifen was administered 20 mg/day and anastrozole was administered 1.0 mg/day. The postmenopausal status was defined as an amenorrhea duration of more than 1 year or serum FSH (follicular stimulating hormone) levels of >40 mIU/ml before primary surgery. Endometrial and ovarian evaluation was performed by Transvaginal Ultrasonography (TU) before the start of hormonal therapy and the changes were periodically measured by TU at an interval of 6 or 12 months. All patients underwent TU assessment of the endometrial lining by measuring the maximum thickness from the outermost limits of endometrial-myometrial juncture. A double-layered endometrial stripe subsequently measuring more than 5 mm at a periodic checkup was considered abnormal and an endometrial biopsy was performed. Ovarian cysts were identified as sonolucencies in the ovary with a diameter of >30 mm in all women.
All statistical analyses were performed using SPSS 15.0 for Windows. Comparative analyses were performed with Kruskal Wallis test, Mann-Whitney U-test, Chi-square test and Fisher's exact test. Continuous variables were presented as mean and standard deviation. Only p-values <0.05 were considered significant.
RESULTS
The mean age of the three groups was 41.7±5.6, 56.1±7.8, and 53.3±7.4 years, respectively. The mean duration of follow-up was 20.6±6.6 months (range, 12 to 36). There was no difference of mean endometrial thickness before hormonal therapy among the three groups (3.72±1.92 vs. 3.45±1.09 vs. 3.06±0.24 mm, Table 1).
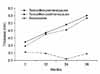
The endometrial thickness was continuously increased in proportion to the duration of receiving tamoxifen from 3.72±1.92 and 3.45±1.09 at baseline to 4.35±2.50 and 4.26±2.15 after 1 year, to 4.89±2.73 and 4.54±1.77 after 2 years, and to 5.50±3.07 and 5.33±2.94 after 3 years in group 1 and group 2, respectively, while it remained <5 mm in group 3 treated with anastrozole for 3 years (p<0.05) (Fig. 1).
Endometrial biopsies were performed for 28 women receiving tamoxifen in whom endometrial pathology suspected; in group 1 (21 women, 13.5%) and group 2 (7 women, 21.9%). Of the 21 women in group 1 undergoing endometrial biopsy, endometrial polyps were found in 6 cases, proliferative endometrium in 7 cases, submucosal myoma in 1 case, simple hyperplasia in 1 case, and atrophic endometrium in 6 cases. Of the 7 women in the group 2, endometrial polyp was found in 1 case and atrophic endometrium in 6 cases. The most common histologic finding was proliferative endometrium in group 1 (7/21 cases, 33.3%) and atrophic endometrium in group 2 (6/7 cases, 85.7%). There was no cases of endometrial cancer in both groups (Table 2).
Ovarian cyst was found by transvaginal ultrasonography during follow up in 30 women (19.4%) of group 1, 2 women (6.3%) of group 2, and 1 woman (5.0%) of group 3. All the cysts were 30-60 mm in size and unilocular or bilocular in shape without any solid portions. Further evaluation such as laparoscopic biopsy was not performed because the ovarian cysts had a benign nature on ultrasonography in all cases.
DISCUSSION
Treatment for women with early and advanced breast cancer are strongly related to the presence of ER-positive and/or PR-positive tumors, which indicates that the estrogen stimulates tumor growth, and that hormonal therapy may be effective in preventing disease progression. Until recently, tamoxifen, which acts by blocking estrogen stimulation, has been known to be an effective adjuvant therapy for breast cancer in pre- and post-menopausal patients with ER-positive breast cancer. However, it is now widely accepted that an AIs should be the treatment of choice for postmenopausal women in the advanced breast cancer setting.10
A trial of AIs as first-line therapy for postmenopausal women with hormone receptor positive advanced breast cancer have shown anastrozole to be at least equivalent to tamoxifen in efficacy and tolerability.9 Multiple phase III trials of AIs for the treatment of advanced breast cancer have demonstrated that letrozole, anastrozole, and exemestane are superior to megestrol as second-line endocrine therapy after failure with tamoxifen.11-15
Unlike tamoxifen, which prevents estrogen binding to its cognate receptor at the DNA level, AIs prevent the formation of estrogen.16 Therefore, they do not have the mixed agonistic/antagonistic properties inherent in tamoxifen, and it is thought that the inhibitors may overcome tamoxifen resistance.
Tamoxifen has an effect on the endometrium that varies with the serum estradiol (E2) concentration in that it will function as an estrogen agonist only in postmenopausal women.17-20 An increased risk of endometrial carcinoma has been described, specifically in postmenopausal women, and the risk increases with cumulative dose and duration of tamoxifen treatment.6,21-25
Cheng et al. compared the endometrial findings of pre- and post-menopausal women receiving tamoxifen therapy with abnormal bleeding.26 No differences were detected in mean endometrial thickness, uterine size, and histopathologic findings in premenopausal patients, regardless of tamoxifen ingestion. In addition, in premenopausal women using tamoxifen in a chemoprevention trial, who had elevated serum levels of E2 because of ovarian stimulation, the endometrial thickness was not increased, suggesting an antiestrogenic effect of tamoxifen on the endometrium in an estrogen-rich environment.27 Although data in the literature are scarce and longer follow-up is needed, initial studies show no adverse effect of tamoxifen on the endometrium in premenopausal women.
In a chemoprevention trial by Chang et al, endometrial carcinoma has been reported in women who were premenopausal at the start of tamoxifen and who became amenorrheic during long-term tamoxifen treatment with proved low serum estrogen levels. Ultrasonography of the endometrium in those women on tamoxifen showed an increased endometrial thickness.27 Only in women with a low serum level of E2, tamoxifen is associated with increased endometrial thickness and increased uterine size on ultrasound, and increased frequency of endometrial pathology.4,27
Tamoxifen can stimulate proliferation of the endometrium, which increases the risk of polyps, hyperplasia, and endometrial cancer by 2- to 4-fold, compared with patients not receiving tamoxifen.6,21-24,28-31 It has been reported that 10% of tamoxifen-treated patients will develop tamoxifen-induced endometrial pathology within 5 years, leading to operative intention.32 Although endometrial cancer was not detected in our data, the change of endometrium in the pre- and post-menopausal women receiving tamoxifen was in accordance with these reports.
In a randomized study (ATAC study) which compared adjuvant anastrozole with tamoxifen in the treatment of menopausal patients with ER positive breast cancer, a lower prevalence of endometrial cancer was found.33 The results of the ATAC endometrial sub-protocol, initiated in order to establish the background prevalence of endometrial pathology and finalized to prospectively assess the incidence of endometrial changes following the start of anastrozole therapy, have been recently published.34,35 Sixty nine patients were assessable after 24 months of therapy with anastrozole and there was no change in the median endometrial thickness compared with the baseline. However, the emerging rate of endometrial pathology did not differ significantly between the patients treated with anastrozole (8.7%) and tamoxifen (17.9%). Similarly, we showed changes from the baseline endometrial thickness after 3 years in women treated with tamoxifen, whereas endometrial thickening did not change in postmenopausal women treated with anastrozole.
The mechanism of action of tamoxifen in stimulating the development of ovarian cysts is not yet fully known. It is believed that tamoxifen competes with estrogen receptors, leading to a decline in circulating estrogen levels and thus increasing the level of gonadotropin releasing hormone, which stimulates the pituitary gonadotropins.36 Chronic treatment with tamoxifen in pre-menopausal women with primary breast cancer has been reported to cause an increase in ovarian estrogen synthesis.37,38 Powles et al.39 demonstrated in a placebo-controlled tamoxifen chemoprevention trial in 1,054 healthy pre- and post-menopausal women, a significantly increased risk of ovarian cysts in pre-menopausal women who had received tamoxifen for >3 months. We found ovarian cyst in 19.4% of pre-menopausal women using tamoxifen in this study. Christensen et al. reported that among the overall population of 428 gynecologically healthy women, 29 (7%, ages 16-43) were found to have ovarian cysts.40
In this study, there were significant changes of endometrial thickness and ovarian cyst formation in women undergoing adjuvant hormonal therapy after breast cancer surgery. When compared with anastrozole, tamoxifen led to much thicker endometrium after 3 years of medication. Additionally, premenopausal tamoxifen users had a higher proportion of ovarian cyst formation than others. Therefore we conclude that all breast cancer patients being treated with hormones should be under close gynecological and ultrasonographic surveillance. Gynecologists must be familiar with this side effect of hormonal therapy to avoid unnecessary invasive studies.


 XML Download
XML Download