

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Primary treatment for women with advanced epithelial ovarian cancer consists of cytoreductive surgery and postoperative platinum and taxane-based combination chemotherapy.1 Despite the primary treatment, the disease will ultimately recur in the majority of cases and the expected 5-year survival rate will not exceed 30-50%.1,2 It would be valuable in optimizing therapeutic management to identify early indicators of the response to chemotherapy. Serum CA-125 assay plays a major role in the management of patients with ovarian cancer because serial antigen measurements reflect the disease course during and after chemotherapy.3 Several authors have explored the clinical significance of serum CA-125 changes during the early postoperative period, but there is still no agreement regarding the prognostic value of post-operative CA-125.4-6 The clinical significance of serum CA-125 decline immediately after primary cytoreductive surgery is uncertain. Furthermore, the relationship between postoperative declines of serum CA-125 and survival has not been clearly defined yet.
The purpose of this study was to evaluate whether the decline in serum CA-125 levels immediately following primary cytoreductive surgery prior to starting adjuvant chemotherapy has a prognostic value in patients with stage IIIC/IV ovarian carcinoma.
Materials and Methods
A retrospective review was conducted of all patients with stage IIIC/IV ovarian carcinoma who underwent primary cytoreductive surgery followed by intravenous platinum-based chemotherapy at our institution from 1994 to 2007. Patients were included if two CA-125 levels were available in the preoperative and immediate postoperative period within one week prior to starting their first chemotherapy cycle. Patients whose postoperative CA-125 level was elevated were excluded.
Demographic, pathologic, treatment, and survival data were collected. The maximum residual tumor size was related to the largest diameter of the largest residual tumor lesion. It was determined by the surgeon during the operation. Percentage decline of CA-125 was calculated on the bases of the formula "[1-(post-operative CA-125/pre-operative CA-125)]×100" as suggested by Brand and Lidor.7 Patients were compared with standard statistical tests in groups by 25% declination intervals.
The primary study end point was to determine if percentage decline of serum CA-125 is a predictor of progression-free survival (PFS). PFS was defined as the time elapsed from the date of the surgery to the date of clinically proven recurrence. Overall survival (OS) was calculated from the date of the surgery to the date of cancer-related death. Since the postoperative CA-125 distribution was not Gaussian, non-parametric statistics were applied. The Chi-square test was used for comparison of observed frequencies. Univariate survival analyses were performed using the Kaplan-Meier method and log-rank test. Cox's proportional hazard model was used for multivariate survival analyses. For all statistical tests, the level of significance was p≤0.05. Statistical software used was SPSS 11.0 (SPSS Inc., Chicago, IL).
Results
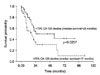
The patient characteristics are described in Table 1. We identified 81 of 112 patients who met the inclusion criteria. In the study group, the median age was 52 years (range: 29-74). Patients were predominantly stage IIIC (n=69, 85.2%) with a minority being stage IV (n=12, 14.8%). The majority of patients had serous histology (n=60, 74.1%). All patients received platinum-based primary intravenous treatment. The number of patients with ≤1 cm residual disease was 54 (66.7%). The median preoperative CA-125 level was 1150.0 U/ml (range: 25.9-21677.0). The median time from primary cytoreductive surgery to postoperative serum CA-125 sampling was 16 days (range: 7-42). The median follow-up time of the survivors was 27.0 months (range: 1.3-143.7), and the median postoperative decline in serum CA-125 levels after cytoreduction was 75% (range: 3.9-99.3%). The median DFSs of each group are shown in Table 2. A ≥75% decline was associated with a median progression-free survival of 25.6 months (95% CI=0-63). This was significantly longer when compared with lesser decline (<75%, p=0.0257, Fig. 1). There were no differences in the overall survival (Data not shown).
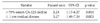
In the multivariate Cox regression model, ≥75% decline of CA-125 levels was an independent predictor of PFS (HR: 2.23; 95%CI, 1.17-4.27, p=0.015) as in shown Table 3. Other significant factor studied was presence of ≤1 cm residual disease. The age, grade, histology, stage and preoperative CA-125 levels were not statistically significant and thus excluded from the model.
Discussion
In our study, ≥75% postoperative decline of CA-125 was associated with pogression-free survival in patients with advanced stage ovarian carcinoma. This finding may be useful to predicting the disease course in early period of the treatment. It is well known that survival outcome of patients affected by advanced ovarian cancer primarily depends on the volume of residual disease after primary surgery,8 and residual tumor ≤1 cm in maximal diameter has been defined as an optimal cytoreductive procedure by the Gynecologic Oncology Group (GOG). In this study, there was no correlation between the postoperative decline in serum CA-125 and residual disease. Each was an independent factor of progression free survival. Postoperative CA-125 decline was not associated with overall survival. The reason for this may be that it has a relatively weak impact on survival or that the following chemotherapies have changed the disease course. It is obvious that the minimal residual disease before chemotherapy is a potent indicator of good prognosis, and the implication concerning the current analysis is that the decreased tumor burden caused by cytoreductive surgery (optimal or not) may have clinical importance, at least in terms of progression-free survival. However, the chemically estimated "decreased tumor burden" may not necessarily be optimal debulking. Brand and Lidor7 found that by using the ratio of CA-125 levels before and after cytoreductive surgery, one can predict the likelihood that the patient was left with less than 2.0 cm residual disease. Conversely, Yedema et al.9 observed that CA-125 levels in the early postoperative period (median time of 5 days) do not always reflect the outcome of cytoreduction. Preoperative CA-125 levels reflect the initial load of CA-125-secreting cells.10 The surgical procedure is able to exert contrasting effects on CA-125 levels. In fact, tumor debulking and drainage of ascites causes a fall in CA-125 levels, whereas peritoneal damage and surgical manipulation of the tumor causes an increase in antigen concentrations.9,11,12 The latter phenomena may disrupt the effect of surgery on changing CA-125 levels. Because the natural half life of CA-125 appears to be approximately 4.8 days,13 the CA-125 level during the immediate postoperative period seems to be influenced by other variable factors besides the reduced volume of tumor tissue.14 Therefore, it was our opinion that it would be better to measure the CA-125 level immediate prior to the first adjuvant chemotherapy, rather than in the early immediate postoperative period. In the current study, the median time from primary cytoreductive surgery to postoperative serum CA-125 sampling was 16 days (range: 7-42). By allowing the interval between the debulking surgery and CA-125 sampling time, the decline of CA-125 level would more accurately reflect the decreased tumor burden by the cytoreduction.
Decades have passed since the CA-125 monoclonal antibody was first isolated by Bast et al.15 It is now widely accepted that the tumor maker CA-125 is a predictive and prognostic factor in CA-125 positive ovarian cancers.16,17 Although more than 2000 articles have been published concerning laboratory and clinical studies of CA125,18 it is difficult to find studies which have analyzed the relationship between survival and the rate of postoperative decline of CA-125.
In conclusion, ≥75% decline of CA-125 may reflect the decrease of tumor burden enough to affect the progression- free survival. If confirmed in prospective studies, these findings suggest that the initial drop in CA-125 after primary surgery may allow a subset of patients with better outcomes to be identified prior to starting chemotherapy. This may have a clinical relevance in the management of patients with advanced ovarian cancer, and may be useful for patient counseling and risk stratification during subsequent clinical trials.


 XML Download
XML Download