

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The treatment choice for patients with gastric cancer is radical gastrectomy with esophagojejunal anastomosis and lymphadenectomy when involves to upper body or cardia of the stomach. Anastomotic leaks are life-threatening complications that can increase postoperative mortality. In total gastrectomy, anastomotic leaks are more common than subtotal gastrectomy, with reported incidence rates ranging from 4% to 17%. The mortality rate is still high (12% to 50%) despite traditional standard management such as conservative treatment with nil per os (NPO), abscess drainage, and re-exploration with surgical repair [123]. Subsequent surgical repair is difficult in patients with anastomotic leaks because of the associated high operative mortality.
Endoscopic self-expandable metal stent (SEMS) replacement has recently begun to be accepted as a primary treatment of patients with esophagojejunal anastomotic leaks after total gastrectomy. Endoscopic SEMS replacement has 2 significant problems: embedded stents due to tissue hyperplasia and stent migration in the patient with anastomotic leaks. Endoscopists should carefully choose the type of SEMS to avoid these issues. Some endoscopists may prefer to use a partially covered SEMS to prevent migration and reduce leakage between the stent and esophageal wall. However, embedded stents are emerging as a common obstacle that can be difficult to extract when using partially covered SEMS and even a conventional fully covered SEMS. Embedded stents may occur with other issues including secondary stricture, perforation, and bleeding, despite the successful removal of stents using various methods [45]. Choosing the right type of stent to avoiding stent migration and embedding is crucial to improve successful endoscopic treatment in patients with anastomotic leaks. Conventional fully and partially covered SEMS may not be suitable considering migration and embedding for endoscopic treatment.
In this study, we used a benign fully covered SEMS with an anchoring thread and thick silicone covering membrane to prevent stents from becoming embedded and migrating in patients with gastric cancer and esophagojejunal anastomotic leaks after total gastrectomy. The clinical outcomes, including effectiveness and complications, were evaluated.
MATERIALS AND METHODS
Patient selection
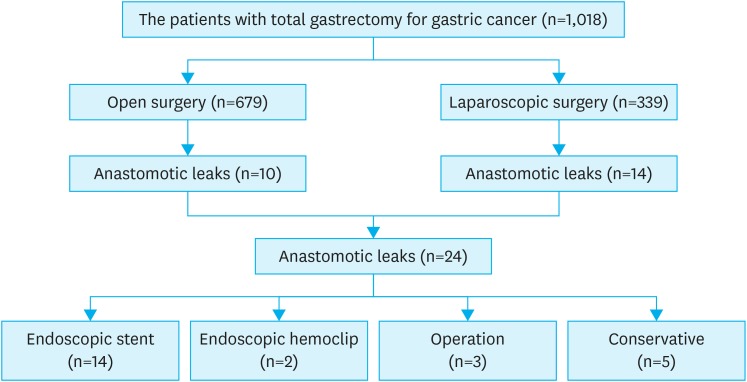
We performed a retrospective review of the data of patients who underwent benign fully covered SEMS placement with the Shim's technique for anastomotic leaks after total gastrectomy to treat gastric cancer between January 2009 and December 2016 at the Chonnam National University Hwasun Hospital. Overall, 1,018 patients with gastric cancer underwent total gastrectomy; anastomotic leaks occurred in 24 (2.4%) cases. Open surgery was performed in 679 cases, including 10 (1.5%) anastomotic leaks, and laparoscopic surgery was performed in 339 cases, including 14 (4.1%) anastomotic leaks. Anastomotic leak treatment included endoscopic stent replacement (n=14, 58.3%), endoscopic hemoclips (n=2, 8.3%), surgical repair (n=3, 12.5%), and conservative treatment (n=5, 20.8%). Of these patients, 14 were enrolled in this study (Fig. 1). We obtained consent from all patients and the study was approved by the Institutional Review Board of the Chonnam National University Medical School, Gwangju, Korea (CNUHH-2015-113).
Embedded stent and migration
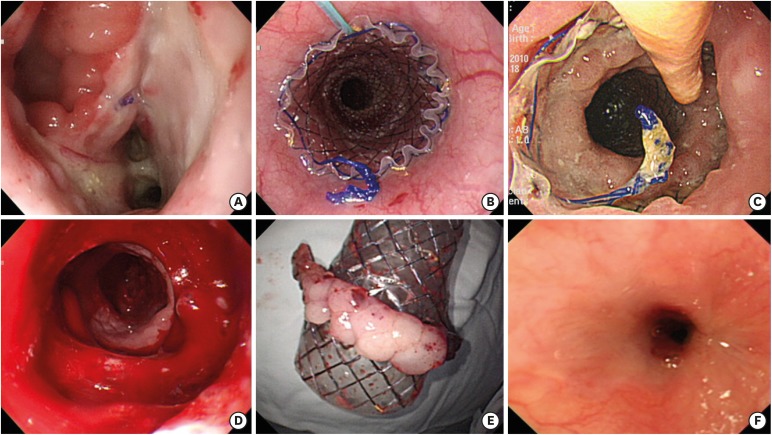
Conventional fully covered SEMS with anchoring thread has been commonly used endoscopic stent for treating esophagojejunal anastomotic leaks after total gastrectomy in Korea. However, this stent can cause embedding into esophageal mucosa by granulation tissue before extraction of stent. We had experience case of anastomotic leaks with a severely embedded stent after use of a conventional fully covered SEMS (Hanarostent®; M.I. Tech, Seoul, Korea). The embedded stent was removed with great difficultly. The rat tooth grasped at the distal end of stent, and the stent was peeled backward through the inner side of the stent under fluoroscopic control. This patient's leaks resolved after stent retrieval, but severe stricture occurred mid-esophagus. The patient ultimately underwent a second surgery for severe stricture after 1 year because of a persistent stricture despite repeated endoscopic balloon dilation (Fig. 2).
Fig. 2
Embedded stent was a major complication after the use of a conventional fully SEMS in a patient with leaks. (A) Large dehiscence at esophagojejunal anastomosis site after total gastrectomy. (B) Endoscopic placement of conventional fully SEMS. (C) Severe circumferential embedded stent after 4 weeks. (D) The stent was removed with difficulty under endoscopic and fluoroscopic guide. (E) Removed stent with attaching hyperplastic mucosa at compressed area. (F) Delayed severe stricture developed at mid esophagus with refractoriness to repeated endoscopic balloon dilatation. The patient finally underwent a second operation after 1 year.
SEMS, self-expandable metal stent.
Fully covered SEMS with an anchoring thread and thick covering membrane
We used a benign fully covered SEMS with a thick membrane and a silk thread (benign Hanarostent®, fully covered esophageal SEMS with Shim' technique; M.I. Tech) to treat anastomotic leaks in the next patient. This stent has a specially designed silicone membrane that was modified in thickness (0.2–0.24 mm) and a long end of the silicone membrane (5 mm) to prevent overgrowth and ingrowth of granulation tissue. This stent was also applied with an anchoring thread, using the so called Shim's technique to prevent migration [6]. The Shim's technique involves attaching the silk thread at the proximal end of the stent, which can then be moved through the nose and attached to the ear lobe with tape, similar to the method for endoscopic nasobiliary drainage.
Endoscopic stent replacement
Anastomotic leaks were diagnosed via esophagram using gastrografin or endoscopy. Abdominal and chest computed tomographies (CTs) were performed to evaluate fluid collection or abscess formation in the abdomen or chest cavity. Endoscopic benign stent placements were performed for the following indications: 1) endoscopic confirmed leaks at esophagojejunal anastomosis site, 2) hemodynamically stable patients with systolic blood pressure greater than 90 mmHg, and 3) no residual cancer after total gastrectomy. The methods used for endoscopic stent replacement are described in Fig. 3. Patients were consciously sedated with intravenous midazolam and fentanyl during the procedure. The stent length was 4 cm longer than the size of the leaks to ensure sufficient coverage of the esophageal and jejunal margins of leakage sites. The stent was carefully deployed to locate the middle portion of the stent at the leakage site through a guide wire under endoscopic and fluoroscopic control. After stent deployment, the silk thread was removed through the nose and fixed to the patient's ear lobe using tape. Simple chest radiography was checked to confirm the stent position the day after the procedure and then at 1-week intervals. Per-oral intake began with a small amount of liquid, which then progressed to a regular diet. If an abscess or fluid collection was found on abdominal or chest CT, abscess drainage was performed with intravenous broad-spectrum antibiotics. Follow-up endoscopy was performed to check the healing status of the leak site and stent position within 3 weeks based on the results of simple chest radiography and clinical findings. The endoscopist can directly observe the healing status of anastomotic leaks through the space between stent and esophageal lumen without embedding stent. In malnourished patients, an additional feeding tube was inserted within stent under endoscopic guidance to improve nutritional status and decrease the incidence of leakage in the space between the esophageal wall and the stent. All stents were extracted with/without a fluoroscopic guide after checking complete closure or other complications under endoscopic visualization. Follow-up endoscopy was scheduled 3–6 months after leak closures, and then at yearly intervals.
Fig. 3
Placement of a benign fully covered SEMS with thick membrane and Shim's technique. (A) Large dehiscence at esophagojejunal anastomosis site (B) fully SEMS with thick and long membrane (white arrow) and silk thread (yellow arrow). (C) No leakage after infusion of gastrografin under fluoroscopy. (D) No embedded stent without any tissue hyperplasia after 4 weeks. (E) Near complete sealing of dehiscence in prechecking endoscopy before removal after 4 weeks. (F) The removal of the stent was delayed to 1 week, and the leaks were completely sealed after 5 weeks.
SEMS, self-expandable metal stent.

RESULTS
Baseline characteristics of patients
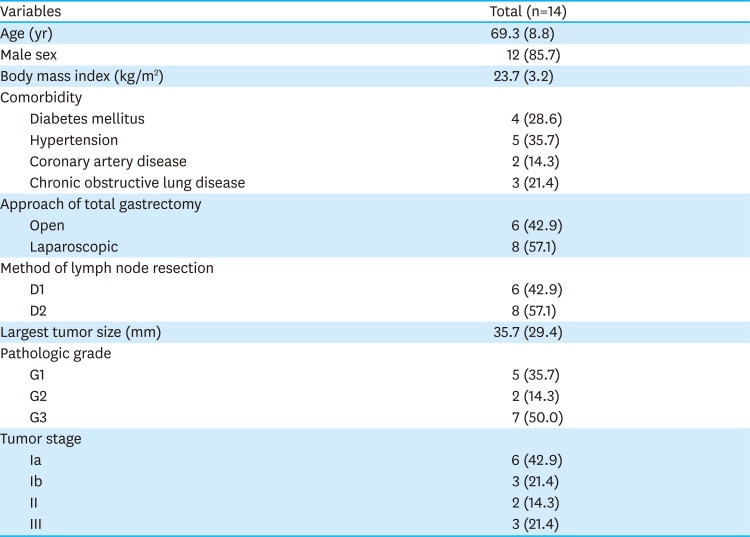
A total of 14 patients underwent endoscopic benign fully covered SEMS placement for esophagojejunal anastomotic leaks after total gastrectomy to treat gastric cancer (Table 1). Patients consistent of 12 (85.7%) men and 2 (14.3%) women with a mean age of 69.3±8.8 years. The mean body mass index was 23.6±3.1. Co-morbidities were hypertension (5, 35.7%), diabetes mellitus (4, 28.6%), coronary artery disease (2, 14.3%), and chronic obstructive lung disease (3, 21.4%). The approaches used for total gastrectomy were open (6, 42.9%) and laparoscopic surgery (8, 57.1%). The mean largest tumor size was 35.7±29.4 mm. Tumor stages were Ia (6, 42.9%), Ib (3, 21.4%), II (2, 14.3%), and III (3, 21.4%)
Table 1
Baseline characteristics of patients with stents for anastomotic leaks after total gastrectomy
Characteristics of anastomotic leaks and endoscopic stent placement
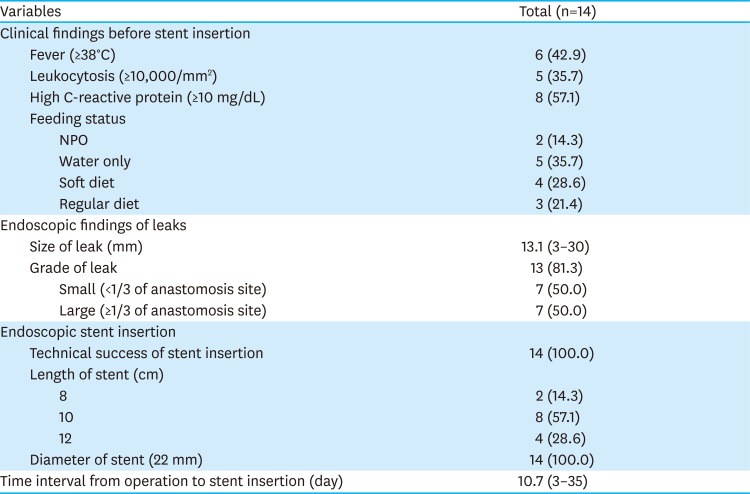
Clinical and endoscopic characteristics are summarized in Table 2. Clinical inflammatory findings of patients were fever (6, 42.9%), leukocytosis (5, 35.7%), and elevated C-reactive protein (8, 57.1%) before endoscopic treatment. The feeding status of patients were NPO (2, 14.3%), sips of water (5, 35.7%), soft diet (4, 28.6%), and regular diet (3, 21.4%) before endoscopic treatment. The mean size of leaks was 13.1 mm (range, 3–30 mm). The duration from operation to stent insertion was 10.7 days (range, 3–35 days). Technical success of stent insertion was achieved in all patients. All patients received benign fully covered SEMS with a thick membrane and a silk thread. The lengths of stent were 8 cm (2, 14.3%), 10 cm (8, 57.1%), and 12 cm (4, 28.6%).
Table 2
Endoscopic and clinical characteristics of anastomotic leakage
Therapeutic outcomes and complications
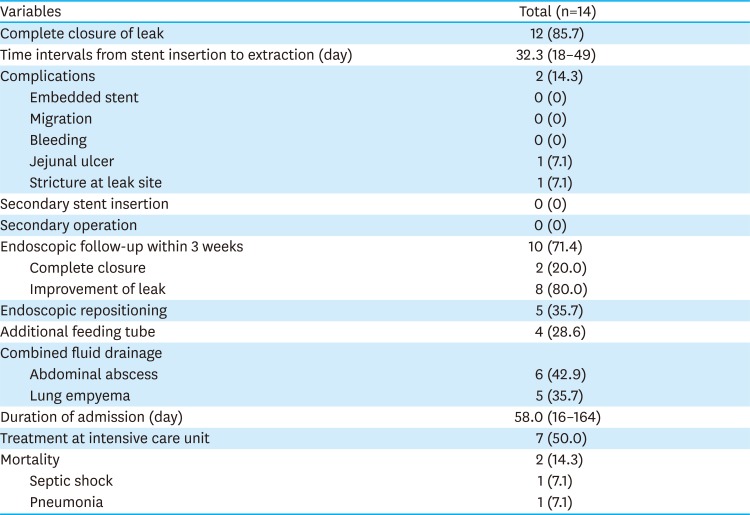
The clinical outcomes and associated variables are summarized in Table 3. Twelve (85.7%) patients had complete resolution from anastomotic leaks after stent extraction, while 2 (14.3%) patients had treatment failure. Two patients died 2 weeks postoperatively, one patient had lung empyema with pneumonia before stent insertion that progressed to acute respiratory distress syndrome, and the other had intraperitoneal abscess that progressed to septic shock. The time interval from stent insertion to extraction was 32.3 days (range, 18–49 days). The overall complication rate was 14.3% (n=2). Embedded stent and migration, which were major complications associated with SEMS, were absent. One patient had a jejunal active ulcer by the distal tip of stent but experienced complete healing after antiulcer treatment. Delayed stricture at large leak area of anastomosis site was found in 1 patient and successfully resolved after repeated endoscopic balloon dilatation.
Table 3
Therapeutic outcomes and complications
Clinical courses after endoscopic stent placement
Per-oral intake was started with a small amount of liquid 24 hours after stent placement, which then progressed to a regular diet. Intravenous broad-spectrum antibiotics were injected in all patients. Combined fluid or abscess drainages were performed for intraperitoneal abscess (6, 42.9%) and lung empyema (5, 35.7%). Improvement of inflammation was seen 2 weeks after stent replacement. Laboratory changes according to endoscopic stent placement are summarized in Table 4. Ten (71.4%) patients received follow-up endoscopy to check the healing status of the leak site and stent position 3 weeks postoperatively. All leaks showed signs of improvement (8, 80.0%) or complete closure (2, 20.0%) under follow-up endoscopy. Endoscopic repositioning was performed in 5 (35.7%) patients due to slight proximal stent displacement. All stents were removed under endoscopy after confirming complete healing of leaks. No additional endoscopic stent placements were needed. Four (28.6%) patients underwent additional feeding tube placement into the deep portion of the jejunum below the stent under endoscopic guidance because of poor appetite and food material remaining in their drainage (Fig. 4).
Table 4
Laboratory changes according to endoscopic stent placement


DISCUSSION
Anastomotic leak after total gastrectomy are more frequent and can be a fatal major complication with a 3-fold higher mortality rate than patient without leaks [7]. Surgical repair has been difficult in patients with anastomotic leaks because of their poor general condition and high mortality. Endoscopic treatment using a SEMS has become widely used as a primary treatment for esophagojejunal anastomotic leaks after total gastrectomy because of its lower invasiveness and favorable outcomes. However, the reported therapeutic efficacy and incidence rates of adverse events of SEMS placement for anastomotic leaks have been inconsistent, with complete closure rates ranging from 23% to 100% [891011]. These variable clinical results for SEMS placement are mainly caused by the type of stent, which influences 2 significant SEMS-related issues: embedded stent due to tissue hyperplasia and stent migration. The endoscopist should consider these issues before choosing the type of stent to be used for treating leaks. The fully covered SEMS with a thick membrane and a silk thread is a novel stent for treating patients with benign condition such as perforation, stricture, and fistula because it can completely prevent tissue hyperplasia and stent migration. To our knowledge, this study is the first clinical study evaluating the feasibility of this stent for treating anastomotic leaks after total gastrectomy in patients with gastric cancer.
Stent migration frequently occurs in patients with anastomotic leaks because no portion of the stent is anchored. The migrated stent may cause secondary severe complications such as obstruction or perforation at the distal bowel, along with sealing failure at the leak site. Higher migration rates have been reported for a fully covered SEMS (26%–87%) compared with a partially covered SEMS (0%–20%) [9101213]. The Shim's technique simply uses a silk thread to prevent the migration of the stent. Using a fully covered SEMS with the Shim's technique was a useful method to completely prevent distal stent migration in all patients. However, the Shim's technique requires the additional process of unthreading through the nose and induced discomfort in some patients.
Embedded stent can occur due to tissue hyperplasia from mucosal irritation at the end portions of the stent. A partially covered SEMS is always associated with embedded stents. The occurrence with a fully covered SEMS is variable, with reported incidence rates ranging from 8% to 21% [1014]. Embedded stents are major adverse events that can increase the difficulty of stent removal when treating patients with benign disease. It can also cause secondary complications including hemorrhage, obstruction, stent fracture, perforation, fistulas, and abscess formation [515]. Tissue hyperplasia or granulation tissue formation is related to the type of stent and the duration of stent placement. Tissue hyperplasia can start to develop during the second week from the insertion of a conventional fully covered SEMS. The stent then becomes completely embedded into the esophageal mucosa by the 4th–6th week. Massive granulation tissue can result in partial esophageal stricture by the 8th week or later [16]. Various methods have been introduced to successfully remove stent in patients with embedded stent, such as stent-in-stent (SIS) technique, argon plasma coagulation, and the overtube technique [4]. Some clinicians prefer to use partially covered SEMS rather than a fully covered SEMS, as the risk for migration is lower, and hyperplasia at the uncovered portion may decrease leakage between the stent and the esophageal wall. Such a stent should still be able to be removed using various removal methods, such as SIS technique despite the occurrence of embedded stent. However, we believe that partially covered SEMS should no longer be used in patients with anastomotic leaks because the novel stent described here can completely prevent stent migration and embedding.
The fully covered SEMS with a thick membrane and a silk thread was first developed in 2007 for treating patients with benign esophageal disease such as stricture. To minimize tissue responses to the stent, a thicker (0.2–0.24 mm) and longer (5 mm) fully covered silicone membrane was used to prevent overgrowth and ingrowth of the granulation tissue. Additionally, the Shim's technique using a silk thread was applied to prevent migration. This clinical study sought to determine the type of stent need to treat anastomotic leaks after total gastrectomy and showed improved complete healing rates without major complications, compared with previous studies using conventional stents [491113]. The novelty of this stent lies in its perfect prevention of the occurrence of distal migration and embedded stent as 2 major problems of conventional stent. In addition, it is possible to safely remove the stent after checking sealing leaks under direct endoscopic view through the space between the esophageal wall and the stent without embedding. The only disadvantage of this stent is the patient's discomfort due to the silk thread coming from the nose (as with a Levin tube). This study was limited in its small sample size and a retrospective study design. Therefore, further investigation is warranted.
In conclusion, the endoscopic placement of a benign fully covered SEMS with a thick membrane and a silk thread is an effective and safe novel treatment for patients with anastomotic leaks total gastrectomy to prevent stent migration and embedding. The endoscopist should carefully choose the type of stent, considering the risk of stent migration and embedding before treating anastomotic leaks.
 XML Download
XML Download